
Schizophrenia: Symptoms, Causes, Diagnosis, Treatment, and Daily Life
Schizophrenia is a serious mental health condition that can affect thinking, emotions, and daily life. This guide explains symptoms such as hallucinations and delusions, early warning signs, causes, diagnosis, treatment options, recovery, and family support, helping readers understand care, improve safety, and support long term stability with confidence.
A change in thoughts, perception, and behavior can be frightening for the person going through it and for everyone around them. Schizophrenia is one of the most misunderstood mental health conditions, yet many people live with it for years while building routines, relationships, and meaningful goals. What helps most is clear information, early care, and steady support.
This condition is not a personality split, and it is not a character flaw. It is a serious mental illness that affects how a person thinks, feels, and relates to reality. Symptoms often begin gradually, which is why families sometimes notice small changes first, such as social withdrawal, sleep problems, suspiciousness, or a drop in school or work performance.
What schizophrenia is, and what it is not
Schizophrenia is a long term mental illness that can affect thinking, emotions, behavior, motivation, and social functioning. During active illness, a person may have hallucinations, delusions, disorganized speech, or disorganized behavior. Some people also have reduced emotional expression, low motivation, and trouble with attention, memory, or planning.
It is important to separate this illness from psychosis and from dissociative identity disorder. Psychosis is a group of symptoms that can happen in several illnesses or medical states. A person can have psychosis and never receive this diagnosis. Schizophrenia is also not the same thing as what people call split personality. That old myth still causes harm and delays care.
Overview and why early care matters
People are often first diagnosed after a first episode of psychosis, usually between the late teen years and around age 30. Signs can appear earlier, sometimes as subtle changes in mood, thinking, or social life. The time before clear psychosis may include isolation, reduced self care, poor concentration, confused speech, or intense suspiciousness.
Early care matters because untreated psychosis is linked with worse health and daily life outcomes. Getting help sooner can improve the long term picture. That does not mean every unusual thought or every difficult teenage phase points to this illness. It means ongoing changes that intensify, interfere with life, or include loss of contact with reality should never be brushed aside.
Symptoms of schizophrenia
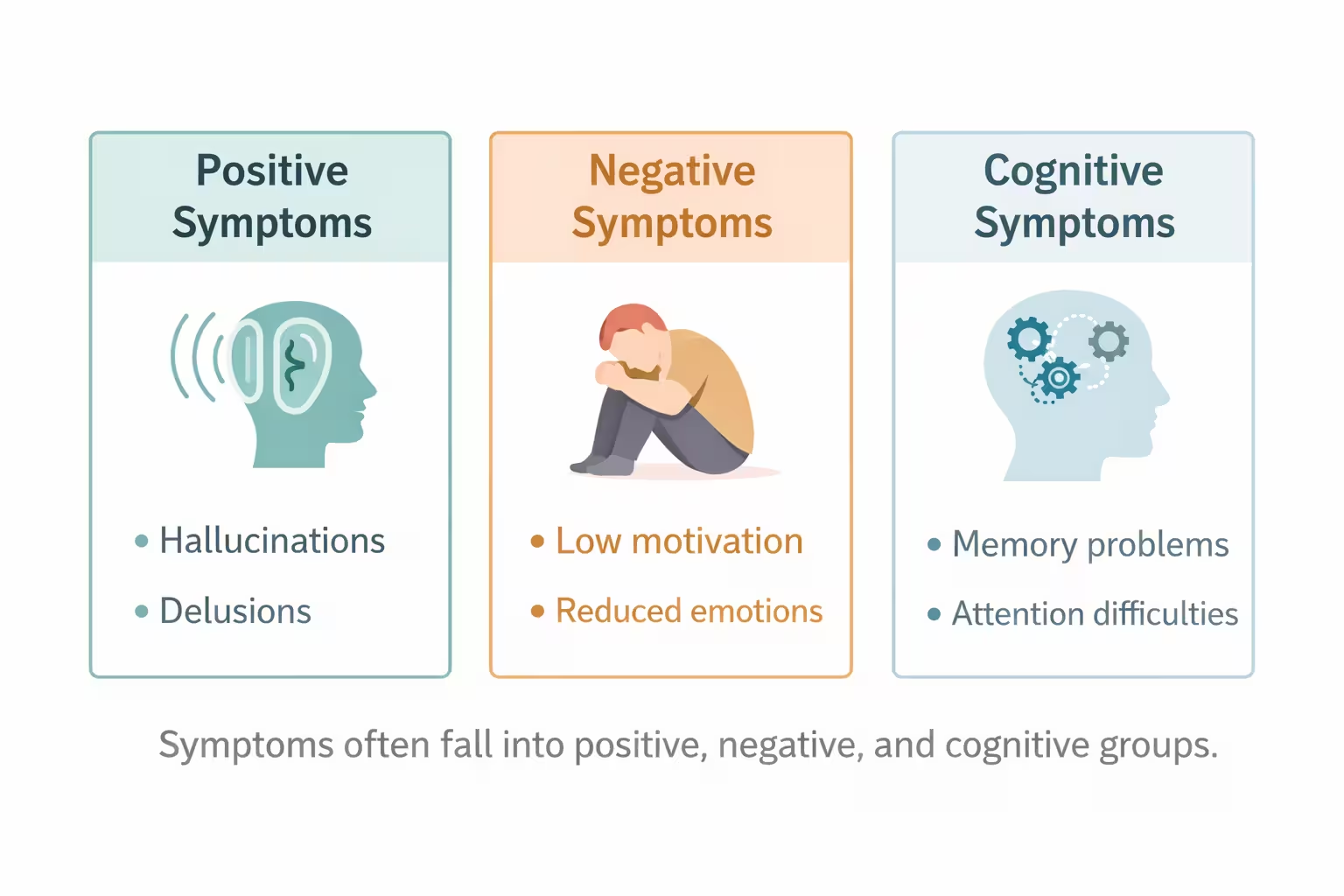
Symptoms are often grouped into positive, negative, and cognitive symptoms. Positive symptoms add experiences that are not usually present. Negative symptoms reduce normal function. Cognitive symptoms affect mental skills that support daily life.
Positive symptoms
Positive symptoms include hallucinations, delusions, and disorganized thinking or speech. Hearing voices is one of the best known symptoms, but hallucinations can involve other senses too. Delusions may include strong false beliefs about being watched, harmed, controlled, or sent secret messages. Some people become very disorganized in conversation or behavior, which can make everyday tasks hard.
Negative symptoms
Negative symptoms can be quieter but just as disabling. A person may show less facial expression, speak less, lose motivation, stop enjoying usual activities, or withdraw from people. These changes are often mistaken for laziness, stubbornness, or depression. In reality, they can be core parts of the illness and often have a major effect on school, work, and relationships.
Cognitive symptoms
Cognitive symptoms are also commonly underexplained. They can include trouble with attention, memory, processing speed, planning, and problem solving. A person may seem distracted, forgetful, or unable to organize simple tasks. These difficulties often show up before a first psychotic episode and can strongly affect independence, even when hallucinations or delusions improve.
Early warning signs in teenagers and young adults
In teenagers and young adults, early signs can blend in with normal stress, which makes them easy to miss. Warning signs may include pulling away from friends, falling grades, sleep disruption, unusual beliefs, confused speech, poor hygiene, irritability, or a sharp drop in motivation.
That does not mean every teen with these signs has this illness. Many mental health and medical problems can look similar at first. What matters is the pattern. If several changes appear together, last for weeks, or keep getting worse, it is wise to seek a professional assessment. Waiting for the problem to become obvious can make the next stage harder to manage.

When to seek urgent help
Some symptoms call for urgent action. Seek emergency help if a person is at immediate risk of harming themselves or someone else, cannot care for basic needs, has severe confusion, or is losing touch with reality in a way that makes them unsafe. In the United States, call or text 988 for suicide and crisis support. Call 911 in a life threatening emergency.
Families often feel torn between respecting independence and responding to danger. A practical rule helps. If safety is uncertain, choose safety first. Stay calm. Use short, simple sentences. Do not argue about whether a belief is true. Focus on getting the person evaluated by a mental health professional or emergency service.
What causes schizophrenia
No single cause explains this illness. Research supports a mix of genetic factors, brain development differences, and environmental influences. Having a family member with the illness can raise risk, but most relatives of affected people do not develop it. Many genes appear to contribute small amounts rather than one gene causing the disorder by itself.
Environmental influences may also matter. Research points to factors such as stressful or dangerous surroundings, poverty, and some exposures before birth, including certain infections or nutritional problems. These factors do not guarantee illness. They only help explain why risk is different from one person to another. In most cases, the condition develops from several influences acting together.
Risk factors and related conditions
The main risk factors include family history, early life adversity, and developmental or environmental stressors. Symptoms often begin earlier in males than in females. Coexisting mental health conditions are also common, including mood disorders, anxiety, and substance use problems. These can cloud the picture and make diagnosis more complicated.
Another important issue is lack of insight, sometimes called anosognosia. Some people do not realize they are ill, even when symptoms are obvious to others. This is not simple denial. It can be part of the illness itself. Recognizing this helps families respond with patience and structure instead of repeated arguments that usually increase mistrust.
How schizophrenia is diagnosed

There is no single blood test, brain scan, or medical test that confirms this diagnosis. Diagnosis is based on a careful clinical assessment by a qualified professional, usually with input from the person and often from family members. The clinician looks at symptoms, duration, level of functioning, and whether another condition could better explain what is happening.
For a diagnosis, symptoms need to persist long enough to meet formal criteria. Current diagnostic standards require a total duration of at least six months, including at least one month of active symptoms. Older subtype labels, such as paranoid or disorganized, are no longer part of current DSM diagnostic criteria. Clinicians also work to rule out other causes, such as substance use, severe mood disorders with psychosis, neurological illness, sleep deprivation, or medication effects.
Conditions that can look similar
Several conditions can resemble it at first. These include bipolar disorder with psychotic features, major depression with psychosis, substance induced psychosis, delirium, some neurological disorders, and schizoaffective disorder. Shorter psychotic illnesses can also occur, including schizophreniform disorder, which resembles it but lasts less than six months.
This is why self-diagnosis from internet lists can go wrong. Two people may both hear voices yet have very different underlying problems and treatment needs. Good assessment takes time and context. It asks what symptoms are present, when they started, what was happening before they began, and how they affect daily life.
Treatment for schizophrenia
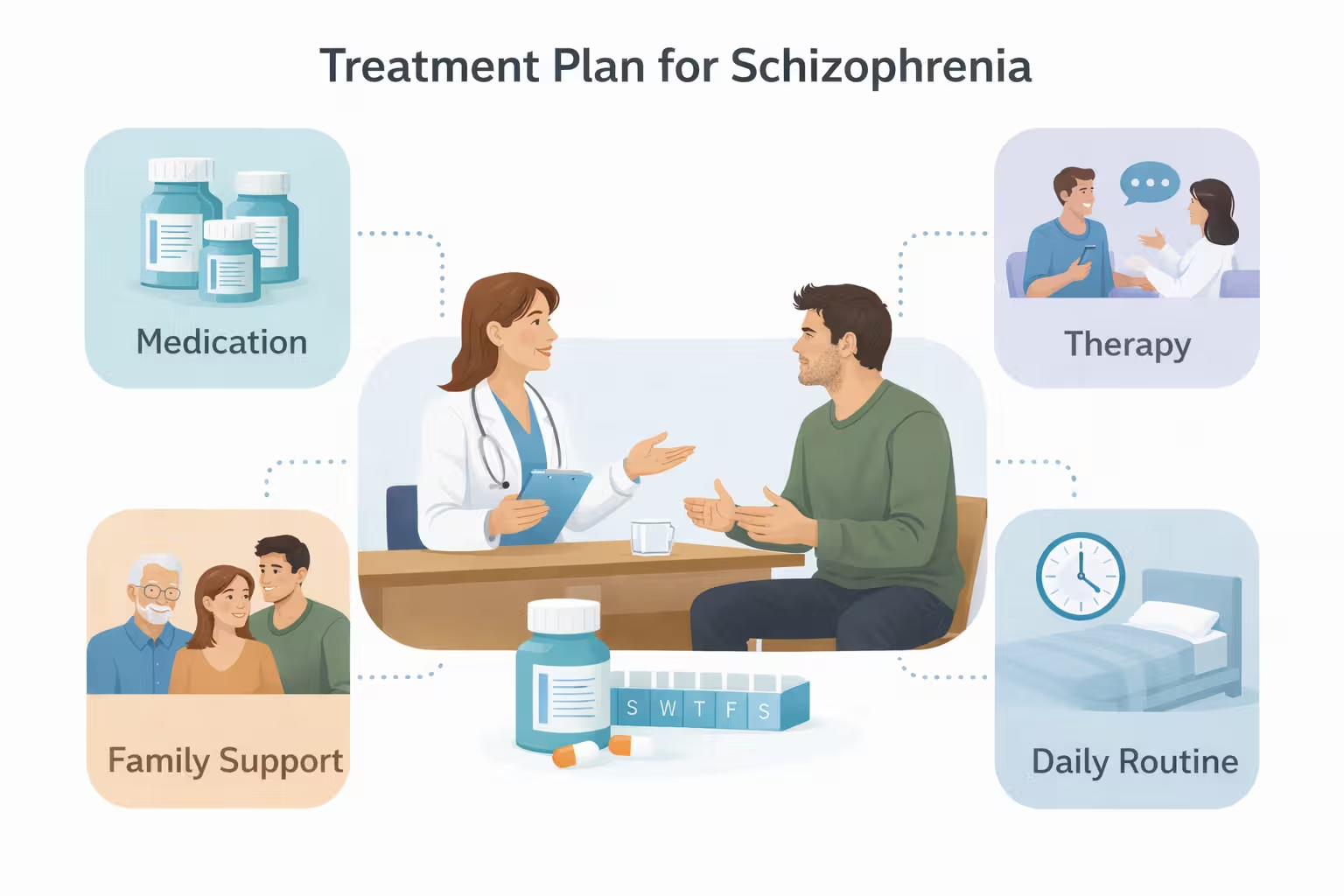
Treatment usually combines medication with psychosocial support. Antipsychotic medication remains a main treatment because it can reduce hallucinations, delusions, and disorganization. Finding the right medicine can take time. Doctors also monitor side effects and may adjust the plan over time rather than relying on a one size fits all approach.
Psychosocial care matters just as much. Helpful supports can include cognitive behavioral therapy for psychosis, family education, skills training, case management, supported education, and supported employment. Daily structure, housing stability, sleep, and substance avoidance also matter. The strongest care plans are person centered and practical, not limited to prescriptions alone.
First episode psychosis and coordinated specialty care
When symptoms first appear, specialized early treatment can change the course of recovery. Coordinated specialty care is a team based model that combines therapy, medication support, family education, school or work support, and shared decision making.
This approach is now considered the standard of care for early psychosis in the United States. It is designed for young people and others in the early stage of illness, when rapid support can protect functioning and reduce long term disruption. If a new diagnosis is being considered, asking about early psychosis programs can be one of the most useful next steps.
Treatment options that deserve more attention
Some people do well with long acting injectable medication, especially if they prefer fewer daily pills or have trouble staying consistent with treatment. This option is part of modern guideline based care and deserves plain language explanation.
Clozapine also needs more attention because it is especially important for treatment resistant illness and for some people with substantial suicide risk. It requires close monitoring, so it is not a casual choice, but it should not be overlooked when standard treatment has not worked well enough. In 2024, the FDA also approved Cobenfy for adults, a newer option with a different mechanism from older dopamine focused treatments for Schizophrenia.
Living with schizophrenia day to day
Life with this illness is not only about symptom control. It is also about sleep, food, appointments, routine, work or school, relationships, and safety. Many people do better with a predictable daily structure. A simple calendar, medication reminders, low stress routines, and regular follow up can lower chaos and help families notice early changes.
Recovery rarely looks like one straight line. Some people have long stable periods. Others have setbacks and then improve again. The most useful goal is often steady function rather than perfection. That can mean keeping appointments, finishing a class, returning to part time work, rebuilding trust at home, or learning early warning signs of relapse before a crisis starts.
Management and support for families facing schizophrenia
Families often need guidance that goes beyond kindness. The most effective support is calm, consistent, and concrete. Learn the person’s warning signs. Help with appointments. Keep a written list of medicines, allergies, doctors, and crisis contacts. Encourage sleep and reduced substance use. Create a crisis plan before a crisis happens.

Helpful communication can be simple:
• Speak slowly and use short sentences.
• Do not mock, challenge, or intensify delusional beliefs.
• Focus on feelings and safety, not winning an argument.
• Offer choices when possible, because choice supports trust.
• Take care of your own stress, sleep, and support needs too.
These steps fit closely with family support guidance from Mayo Clinic, NAMI, and MedlinePlus, which all stress encouragement, practical help, patience, and crisis readiness.
Complications and long term outlook in schizophrenia
Without treatment, this illness can lead to serious social and health complications. These may include job loss, housing instability, substance misuse, social isolation, legal problems, poor self care, and medical illness. Suicide risk is higher than average, especially earlier in the course of illness. That is one reason families should take hopelessness, withdrawal, or talk of self harm very seriously.
The long term outlook varies. Some people improve a great deal with treatment and support. Others continue to have ongoing symptoms or cognitive problems that affect independence. Even then, progress is possible. A person can still gain stability, form relationships, and build a life with meaning. Hope is most useful when it is paired with realistic planning, steady care, and respect for the person’s dignity.
Prevention and relapse in schizophrenia
There is no guaranteed way to prevent it. Still, some steps may reduce harm and improve outcomes. The most important are recognizing early changes, seeking assessment early, and staying engaged with treatment once a plan is in place. Prevention, in real life, often means preventing relapse, crisis, and avoidable decline.
What helps most:
- Early evaluation when psychotic symptoms or strong warning signs appear.
- Sticking with treatment even after symptoms ease.
- Avoiding alcohol and recreational drugs when possible.
- Protecting sleep and daily routine.
- Keeping family or trusted supporters involved in the care plan.
These are simple steps, but they align with the strongest advice repeated across major medical sources.
Common myths that need to end
One of the most damaging myths is that this diagnosis means a person is violent. Most people with this illness are not violent. Risk rises more with untreated symptoms or substance misuse, and it falls when treatment and support are in place. Another myth is that this condition means split personality. It does not. These myths increase stigma and can delay help.
A third myth is that insight can be forced by logic. Families sometimes think the right argument will make the person admit what is happening. Often that backfires. Trust, structure, treatment, and patience work better than debate. Clear language and calm support are part of good care.
Conclusion
Schizophrenia is a serious but treatable mental illness. The clearest picture includes more than symptoms and causes. It also includes early warning signs, accurate diagnosis, first episode care, practical treatment choices, daily functioning, and family support.
When someone begins to lose touch with reality, the right response is not fear or blame. It is early assessment, respectful care, and a plan that supports safety and long term function. Good treatment can reduce symptoms, lower crisis risk, and help people move toward a steadier life.