
Depression: Symptoms, Causes, Treatment, and When to Get Help
Depression is one of those words people use loosely, and that causes problems. Feeling low after a bad week is human. Feeling emotionally flat for two days after a loss is also human. A depressive disorder is different. It can change mood, energy, sleep, appetite, concentration, motivation, and the ability to function at work, school, or home. It can also show up physically, not just emotionally. That is why people often miss it in themselves or in someone close to them.
In the United States, this is not a rare issue. NIMH estimated that 21 million U.S. adults had at least one major depressive episode in 2021, and CDC data show that during August 2021 to August 2023, 13.1% of people age 12 and older had depression in a given two-week period. The burden is higher in younger groups, in females, and in lower-income households. That means this is not just a private struggle. It is a major public-health issue that affects families, work, school, and physical health.
What this condition really is, and what it is not
At its core, depression is a mood disorder marked by a persistent low mood, loss of interest or pleasure, or both. For major depression, symptoms generally last for at least two weeks and interfere with daily life. That time threshold matters because it separates a clinical condition from normal emotional swings. It is not a character flaw, laziness, or a lack of discipline. It is also not defined by sadness alone. Some people feel empty, numb, slowed down, or constantly irritated rather than tearful.
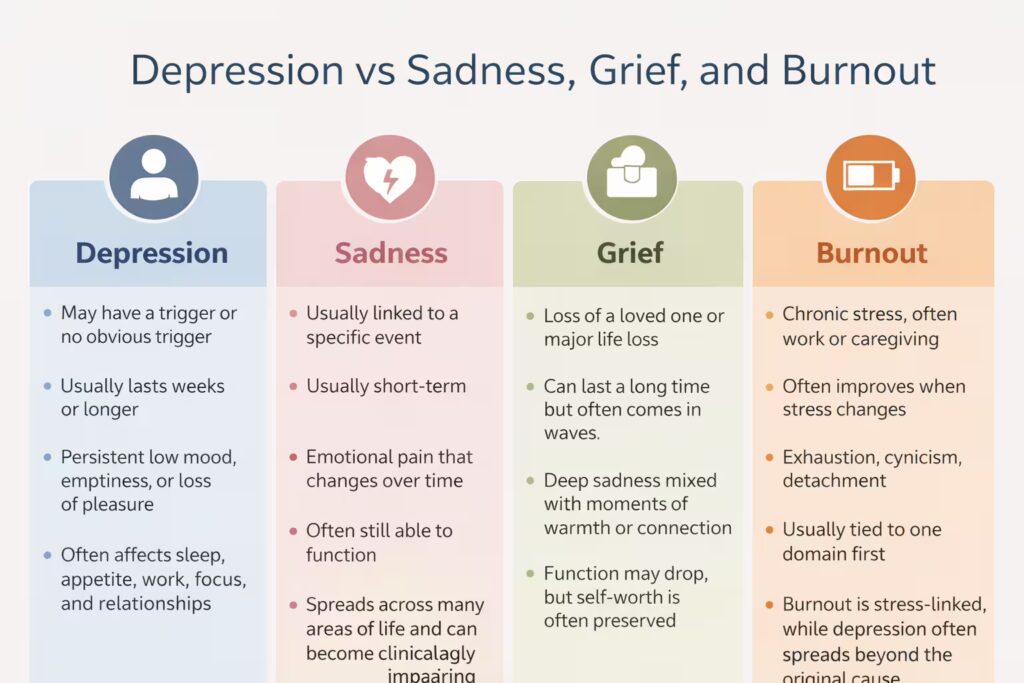
It is also not the same as grief. Grief often comes in waves and may still include moments of warmth, humor, or connection. Major depression tends to be heavier and more constant. In grief, self-esteem is often preserved. In major depression, worthlessness and self-loathing are more common. That distinction matters because people frequently tell themselves they are “just sad” or “just burned out” when the pattern is already clinical and needs proper care.
Burnout can overlap with this condition, but it is not identical either. Burnout is usually tied to chronic stress, often from work or caregiving, and may ease when the stressor changes. A depressive episode tends to spread across life. It affects sleep, appetite, motivation, thinking, relationships, and self-worth even outside the original stress source. If the problem follows you everywhere and keeps shrinking your ability to function, stop calling it “just stress.” That excuse delays treatment.
Common signs people miss
Many people only look for obvious sadness, which is a mistake. This condition can affect emotion, thinking, behavior, and the body at the same time. Someone may look “fine” while struggling with slowed thinking, indecision, low energy, body aches, irritability, or a deadened sense of pleasure. That is one reason it goes untreated for so long. A person can keep working, keep answering messages, and still be clearly unwell.
Emotional and thinking symptoms
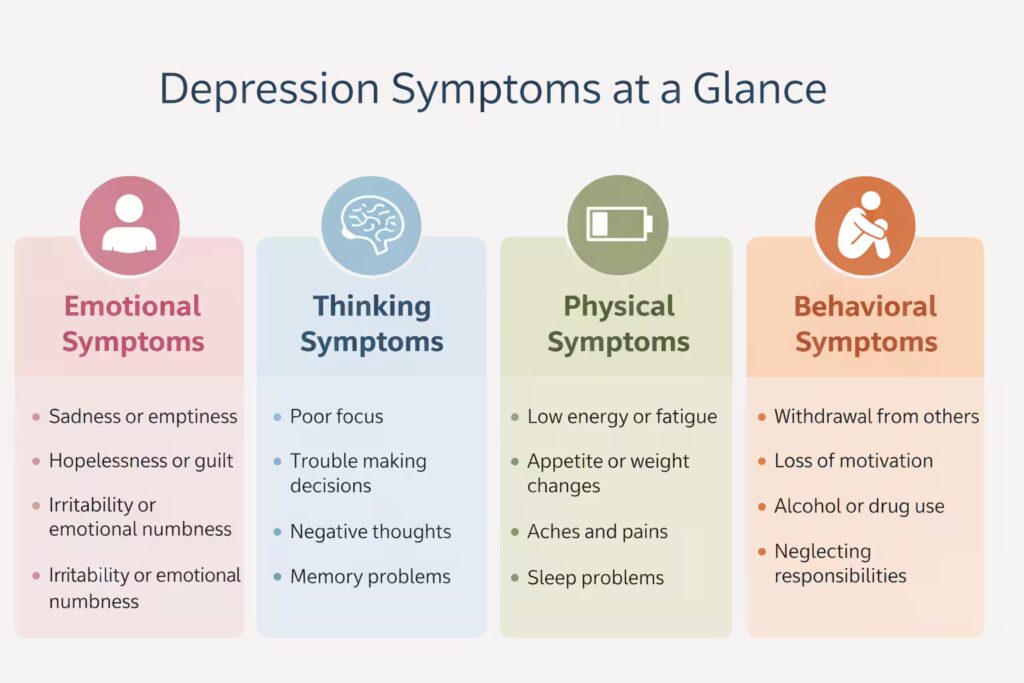
Emotional signs can include sadness, emptiness, hopelessness, guilt, restlessness, frustration, or emotional numbness. Thinking symptoms can include poor focus, memory trouble, indecision, negative bias, rumination, or a constant feeling that nothing will improve. NIMH and other major clinical sources also highlight loss of interest, low energy, and difficulty concentrating as core features. In real life, this may look like abandoning hobbies, avoiding friends, rereading the same sentence six times, or feeling overwhelmed by small decisions.
Physical and behavioral symptoms
This condition also has a physical side that people underestimate. Sleep can go either direction, too little or too much. Appetite can fall or rise. Some people feel slowed down, while others are visibly agitated. Physical aches or pains can also show up without a clear medical explanation. Behaviorally, the signs may include withdrawal, more drinking, missed deadlines, poor self-care, or loss of sexual interest. When the body, mind, and routine all start changing together, that is a serious pattern, not a phase.
Watch for combinations like these:
- Losing interest in activities that used to matter
- Sleeping badly and feeling exhausted anyway
- Eating much more or much less than usual
- Pulling away from people without a clear reason
- Feeling worthless, hopeless, or stuck
- Thinking about death, escape, or not wanting to be here
Those clusters matter more than any single symptom by itself.
Table 1: Symptoms of depression by category
|
Symptom category |
Common signs |
What it may look like |
|
Emotional |
Sadness, emptiness, hopelessness, guilt, numbness |
Feeling flat, crying often, losing interest in life |
|
Thinking |
Poor focus, indecision, memory trouble, negative thoughts |
Struggling at work, rereading the same lines, feeling mentally slow |
|
Physical |
Fatigue, aches, appetite changes, sleep changes |
Oversleeping, insomnia, low energy, unexplained body pain |
|
Behavioral |
Withdrawal, loss of motivation, poor self-care |
Avoiding friends, missing deadlines, neglecting daily routines |
|
Risk-related |
Thoughts of death, self-harm, severe hopelessness |
Talking about escape, feeling trapped, giving up on responsibilities |
How symptoms can look different by age, sex, and culture
One major weakness in many articles is that they describe a single stereotype. Real life is messier. In children, symptoms may include clinginess, irritability, aches and pains, or school refusal. In teens, it may look like anger, drug or alcohol use, self-harm, school decline, oversleeping, or social withdrawal. In older adults, symptoms may be less obvious and may be dismissed as aging, illness, or personality change, which is wrong. Depression is not a normal part of aging.
Sex-linked patterns matter too. U.S. data show higher prevalence in females than males, but that does not mean men are less affected in practical terms. Men may show more irritability, isolation, overwork, reckless coping, or substance use instead of openly saying they feel sad. That means families often miss the condition because they are looking for crying, not withdrawal and anger. Bad assumption. Wrong pattern recognition. Delayed help.
Culture matters as well. The National Institute on Aging notes that in some cultures, low mood may be expressed mainly through physical symptoms such as headaches, digestive issues, cramps, or body pain. That means a person may show up talking about fatigue, stomach trouble, and tension, while the emotional disorder underneath goes unnoticed. Good content should say this plainly, because many people do not realize their body can be carrying part of the story.
|
Group |
How symptoms may show up |
|
Children |
Clinginess, school refusal, aches, irritability |
|
Teens |
Anger, withdrawal, poor school performance, oversleeping |
|
Adults |
Hopelessness, low energy, poor focus, loss of interest |
|
Older adults |
Fatigue, memory complaints, sleep changes, physical symptoms |
Types clinicians talk about
Not every depressive condition is the same. Major depression usually refers to a cluster of symptoms lasting at least two weeks and interfering with normal life. Persistent depressive disorder is generally less intense day to day but lasts much longer, often around two years or more. That longer, lower-grade pattern is dangerous because people can mistake it for their personality and stop expecting life to feel better.
Other forms include seasonal affective disorder, which tends to follow seasonal light changes, and perinatal depression, which can occur during pregnancy or after childbirth. There is also depression with psychotic features, which is more severe and may involve delusions or hallucinations. These are not minor variations. They can change risk level, treatment choice, and the urgency of care.
A critical distinction is bipolar disorder. Bipolar illness includes depressive episodes, but it also involves periods of mania or hypomania. That matters because the treatment approach can differ. If someone has had episodes of unusually high energy, decreased need for sleep, racing thoughts, inflated confidence, or reckless behavior, a clinician has to consider bipolar disorder rather than assuming unipolar depression. Sloppy self-diagnosis here is a bad idea.
Different types of depression
|
Type |
Short explanation |
Common pattern |
|
Major depression |
A depressive episode with significant symptoms lasting at least two weeks |
Strong effect on daily life, mood, and function |
|
Persistent depressive disorder |
Longer-lasting but often less intense symptoms |
Chronic low mood for years in some cases |
|
Seasonal affective disorder |
Symptoms tied to seasonal light changes |
Often worse in late fall and winter |
|
Perinatal depression |
Occurs during pregnancy or after childbirth |
More serious than short-term “baby blues” |
|
Depression with psychotic features |
Severe depression with psychosis symptoms |
May include delusions or hallucinations |
|
Bipolar depression |
Depressive episodes within bipolar disorder |
Must be separated from unipolar depression because treatment differs |
Why it happens
There is no single cause. Major clinical groups describe this condition as the result of interacting biological, psychological, social, and environmental factors. Brain chemistry may play a role. Genetics may increase vulnerability. Stressful life events, trauma, chronic illness, pain, isolation, and substance use can also contribute. Some medications and medical problems can mimic or worsen depressive symptoms, which is why a real assessment matters.
Risk does not mean destiny. A family history raises the chance, but it does not guarantee that someone will develop a disorder. The same is true for poverty, loneliness, grief, or chronic stress. These factors load the system, but people still vary in how they respond. A more accurate way to think about it is this: some people carry more biological or psychological vulnerability, and when enough pressure builds, a depressive episode becomes more likely.
Physical illness can complicate everything. NIMH notes that depressive symptoms can co-occur with conditions like diabetes, cancer, heart disease, and chronic pain, and each can worsen the other. That is one reason people sometimes get trapped in a cycle. Poor sleep worsens pain. Pain worsens mood. Low mood worsens motivation. Motivation drops, treatment slips, and daily life gets smaller. You do not break that loop with motivational quotes. You break it with assessment and treatment.
How diagnosis works
A diagnosis is not based on one sad day or a single online quiz result. Clinicians look at symptom pattern, duration, severity, daily impairment, past history, family history, medication use, substance use, and medical causes that can mimic the condition. Tools such as the PHQ-9 may be used to help assess symptom burden, but screening is not the same as diagnosis. It is one piece of a larger evaluation.
To receive a diagnosis of major depression, a person generally needs five or more symptoms nearly every day for at least two weeks, and one of those symptoms must usually be depressed mood or loss of interest. A good first appointment may include questions about sleep, energy, appetite, concentration, guilt, self-harm thoughts, family history, stressors, and possible manic symptoms. It may also include checking for medical issues such as thyroid problems, medication effects, or substance-related causes.
Treatment that actually helps
This is one of the most treatable mental health conditions, but people still avoid help because they expect a single magic fix. That is not how it works. Treatment usually depends on severity, symptom pattern, history, safety risk, and personal preference. For many people, the best outcomes come from a combination of approaches rather than one tool used badly and inconsistently.
Therapy
Evidence-based psychotherapy is a core treatment. Major clinical sources consistently point to cognitive behavioral therapy, interpersonal therapy, and related structured approaches as effective options. Therapy is not just “talking about feelings.” Good therapy identifies distorted thought patterns, avoidance, relationship stress, routines, and behavioral shutdown. Then it works on them systematically. It also gives people a framework for relapse prevention, not just symptom relief in the moment.
CBT is especially useful when negative thinking and withdrawal keep feeding the episode. Interpersonal therapy can help when the condition is tied closely to loss, role change, conflict, or strained relationships. Family-focused work may also matter in some cases. The point is not to glorify one school of therapy. The point is fit. A strong therapeutic relationship and a structured, evidence-based approach usually matter more than trendy labels.
Medication
Antidepressant medication can help, especially in moderate to severe cases, recurrent episodes, or situations where therapy alone is not enough. This is where people get childish and ideological. One side treats medication like weakness. The other treats it like a shortcut. Both views are dumb. Medication is a tool. It helps some people significantly, helps others partially, and may require dose changes, time, or switching. Clinical guidance also notes that medication may be combined with psychotherapy rather than used alone.
Improvement is not always immediate. People also need monitoring, especially when starting or changing medication. Mayo Clinic notes that anyone taking an antidepressant should be watched for worsening symptoms or unusual behavior, especially early in treatment or after dose changes. That does not mean medication is unsafe by default. It means real treatment includes follow-up, not blind optimism.
Lifestyle and self-management
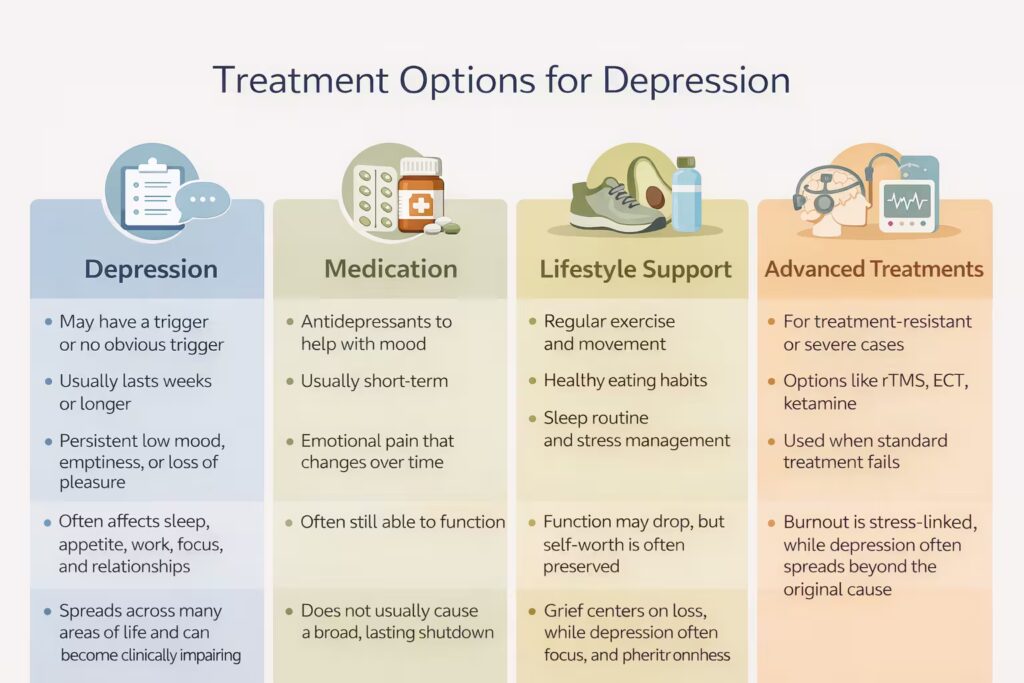
Lifestyle changes are not a substitute for care when symptoms are significant, but they do matter. Major organizations point to regular exercise, sleep routine, less alcohol, healthy eating, and structured daily habits as useful supports. Exercise in particular is often helpful for mood and function. The mistake is treating these as motivational slogans. A person in a real episode may need tiny steps, not perfect routines. Getting out of bed, showering, walking for ten minutes, and eating one stable meal can be a valid starting point.
Telehealth can also widen access, especially for people limited by cost, transportation, caregiving, or stigma. In the U.S., access still remains uneven. NIMH data show that only about 61% of adults with a major depressive episode in 2021 received treatment in the past year, and treatment rates among adolescents were even lower. That gap matters because untreated illness can become more severe, more impairing, and harder to reverse.
Advanced options for difficult cases
When standard treatment does not work well enough, clinicians may consider additional options. NAMI lists brain stimulation therapies such as ECT and rTMS, as well as newer treatments like ketamine and esketamine, as part of the treatment landscape for more severe or treatment-resistant cases. These are not first-line choices for everyone, and they are not casual wellness trends. They are specialist-level options used in the right context.
What to prepare before your first depression appointment
- How long symptoms have been happening
- Whether sleep, appetite, and focus changed
- Any history of mania, hypomania, or psychosis
- Current medications and alcohol or drug use
- Family history of mood disorders
- Major stress, trauma, illness, or loss
- Any thoughts of self-harm or suicide
Treatment options for depression
|
Treatment option |
Best used for |
What it helps with |
Limits or cautions |
|
Cognitive behavioral therapy |
Mild to moderate cases, negative thought cycles, relapse prevention |
Changes thought patterns and behavior |
Needs consistency and a good therapist fit |
|
Interpersonal therapy |
Depression linked to loss, conflict, or life changes |
Improves relationship stress and coping |
Not every therapist offers it |
|
Antidepressant medication |
Moderate to severe or recurrent cases |
Can reduce mood symptoms, improve sleep and function |
May need time, dose changes, or monitoring |
|
Combined therapy and medication |
Moderate to severe cases |
Often stronger than one approach alone |
Requires follow-up and adherence |
|
Exercise and routine support |
Mild symptoms or as part of a broader plan |
Helps energy, sleep, and function |
Not enough alone for severe cases |
|
rTMS, ECT, ketamine or esketamine |
Treatment-resistant or severe cases |
May help when standard treatment fails |
Requires specialist care |
What to expect from treatment
Recovery often happens in layers. Sleep may improve before mood. Concentration may improve before enjoyment returns. A person may stop feeling actively hopeless before they feel motivated again. That uneven pattern is normal. What matters is direction, not immediate perfection. A realistic treatment plan also includes follow-up, side-effect review, a safety plan if needed, and a decision about what to do if the first approach is not enough.
What recovery often looks like
People want a clean timeline, but recovery is rarely neat. Some episodes improve over weeks to months. Some recur. Some people improve with one course of therapy. Others need longer-term care, medication, or a return to treatment after a later relapse. That is not failure. It is how many recurrent illnesses work. The smarter goal is not pretending relapse is impossible. It is learning the earliest warning signs and responding faster next time.
Common early warning signs include social withdrawal, appetite change, rumination, poor sleep, increased irritability, dropping routines, and a return of hopeless or self-critical thinking. Many people wait until the crash is obvious. That is backwards. The right move is to act when the pattern starts, not when it destroys the month. Good long-term care often includes sleep protection, regular appointments when needed, movement, social contact, and a written plan for what to do if symptoms return.
When to seek urgent help

If someone is thinking about self-harm, suicide, or feels unable to stay safe, this stops being a “read an article and think about it” situation. It becomes urgent. In the United States, the 988 Suicide & Crisis Lifeline is available by call, text, or chat for emotional distress, mental health struggles, substance use concerns, or suicidal thoughts. If there is immediate danger or an active attempt, call emergency services right away. Do not leave the person alone if safety is in question.
When to get help for depression
|
Situation |
What to do |
|
Low mood, fatigue, and loss of interest lasting more than two weeks |
Schedule a medical or mental health evaluation |
|
Symptoms are affecting work, school, sleep, or relationships |
Seek professional help soon |
|
Symptoms keep returning after seeming to improve |
Get reassessed instead of waiting for another crash |
|
Alcohol or drug use is getting worse with mood symptoms |
Seek coordinated care |
|
Thoughts of death, suicide, or self-harm |
Get urgent help immediately |
|
Psychosis, inability to stay safe, or extreme deterioration |
Use emergency or crisis services right away |
How to support someone you care about
Trying to “fix” a loved one usually backfires. What helps more is calm, concrete support. Listen without arguing them out of their feelings. Ask direct questions if you are worried, including whether they feel safe. Offer practical help, like booking an appointment, sitting with them during a call, helping with transport, or reducing a few immediate tasks. Passive concern is easy. Useful support takes effort.
A better approach looks like this:
- Say what you have noticed, without judgment
- Avoid lazy lines like “just think positiv
- Encourage professional care, not secrecy
- Stay alert for talk of death, hopelessness, or feeling trapped
- Help reduce access to obvious means of self-harm if risk is rising
- Keep checking in, especially after a crisis or treatment change
This is not about saying the perfect thing. It is about showing up consistently and taking risk seriously.
Frequently Asked Questions
Conclusion
Depression is common, treatable, and far more complex than most people think. It can look emotional, physical, cognitive, or behavioral. It can resemble stress, grief, burnout, pain, or anger. It can show up differently in teens, adults, men, older adults, and across cultures. The biggest mistake is waiting for it to become dramatic before taking it seriously. The smartest move is earlier recognition, proper evaluation, and treatment that matches the real pattern, not the stereotype.