What Is Borderline Personality Disorder? Signs, Diagnosis, and Support
Borderline Personality Disorder is a mental health condition marked by emotional instability, fear of abandonment, impulsive behavior, unstable relationships, identity disturbance, and rapid mood shifts. It often develops from a mix of genetic factors, childhood trauma, and brain based emotional regulation issues. Diagnosis is made by a licensed mental health professional, and treatment usually includes psychotherapy such as dialectical behavior therapy, supportive counseling, and symptom focused care. Around 1.4% of U.S. adults live with borderline personality disorder in a given year.
A person can look calm on the outside and still feel as if everything inside is shifting too fast. A text message goes unanswered. A small disagreement feels crushing. A loving relationship suddenly feels unsafe. For some people, that pattern is not just stress or a bad week. It is a deeper struggle with emotional regulation, self-image, and connection. Borderline personality disorder is one of the clearest examples of that kind of struggle. It can shape how a person feels, reacts, trusts, and recovers after conflict, but it is treatable, and improvement is possible with the right care.
What Borderline Personality Disorder Actually Means
Borderline personality disorder is a mental health condition that strongly affects emotion regulation. It often brings intense reactions, unstable relationships, impulsive behavior, and a shifting sense of self. The condition usually begins in adolescence or early adulthood, and many people first notice that their reactions feel stronger, faster, and harder to control than those of other people around them. It is not a character flaw. It is not attention seeking. It is a serious condition that can disrupt daily life, yet many people improve with structured treatment and long term support.
The name can confuse people. It does not mean someone lives on the edge of sanity. It is an older diagnostic term that stayed in medical use, even though many clinicians and patients focus more on the features behind the label, such as emotional dysregulation, unstable identity, fear of abandonment, and difficulty tolerating distress. Some health systems also use the term “emotionally unstable personality disorder.” What matters most is the actual pattern of symptoms, how long they last, and how much they affect safety, relationships, work, and daily functioning.
Core Symptoms and How They Feel in Real Life
Borderline personality disorder affects far more than mood. It can change how a person interprets events, reads other people, and reacts to stress. A person may feel deeply connected to someone in the morning, rejected by noon, and overwhelmed by shame by evening. These changes are often rapid. They may be triggered by conflict, distance, uncertainty, or fear of being left. Unlike ordinary stress, the response can feel total. Many people describe it as emotional pain that floods the whole body and makes clear thinking hard in the moment.
Clinicians diagnose the condition based on a pattern, not one single symptom. Common features include intense fear of abandonment, unstable and intense relationships, fast shifts in self-image, impulsive behavior, self-injury or suicidal behavior, intense sadness or anxiety, chronic emptiness, strong anger, and brief stress-related paranoia or dissociation. A person does not need every feature. The diagnosis is made when a broader pattern appears over time and causes real impairment.
In daily life, these features often show up in simple moments that do not look simple to the person experiencing them. A canceled plan may feel like rejection. A neutral comment may feel like criticism. Silence may feel like abandonment. That does not mean the person is being dramatic on purpose. It means the nervous system may react to threats more quickly and more intensely than expected, especially in close relationships. This is why the condition often becomes most visible with partners, family, and close friends, rather than with strangers.
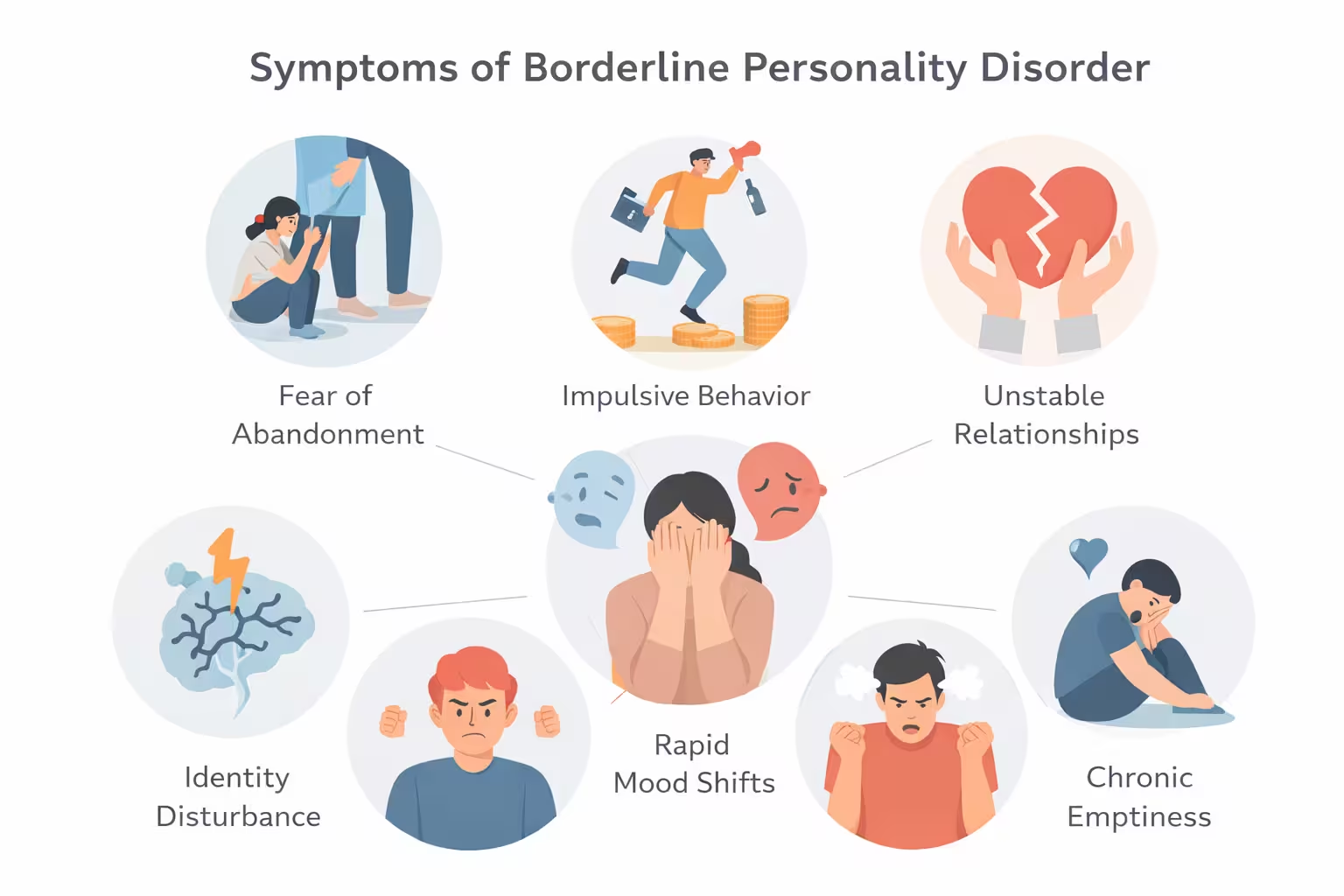
Common symptom patterns include:
- Fear of abandonment, whether the threat is real or imagined
- Unstable relationships, often swinging between closeness and anger
- Identity disturbance, with shifting values, goals, or self-worth
- Impulsive behavior, such as unsafe sex, substance misuse, binge eating, reckless spending, or risky driving
- Self-harm or suicidal behavior, especially during emotional crises
- Chronic emptiness, boredom, or feeling unreal
- Intense anger, shame, or guilt
- Brief dissociation or suspicious thinking under stress
These patterns can vary in intensity from person to person.
What May Cause It and Who Is at Higher Risk
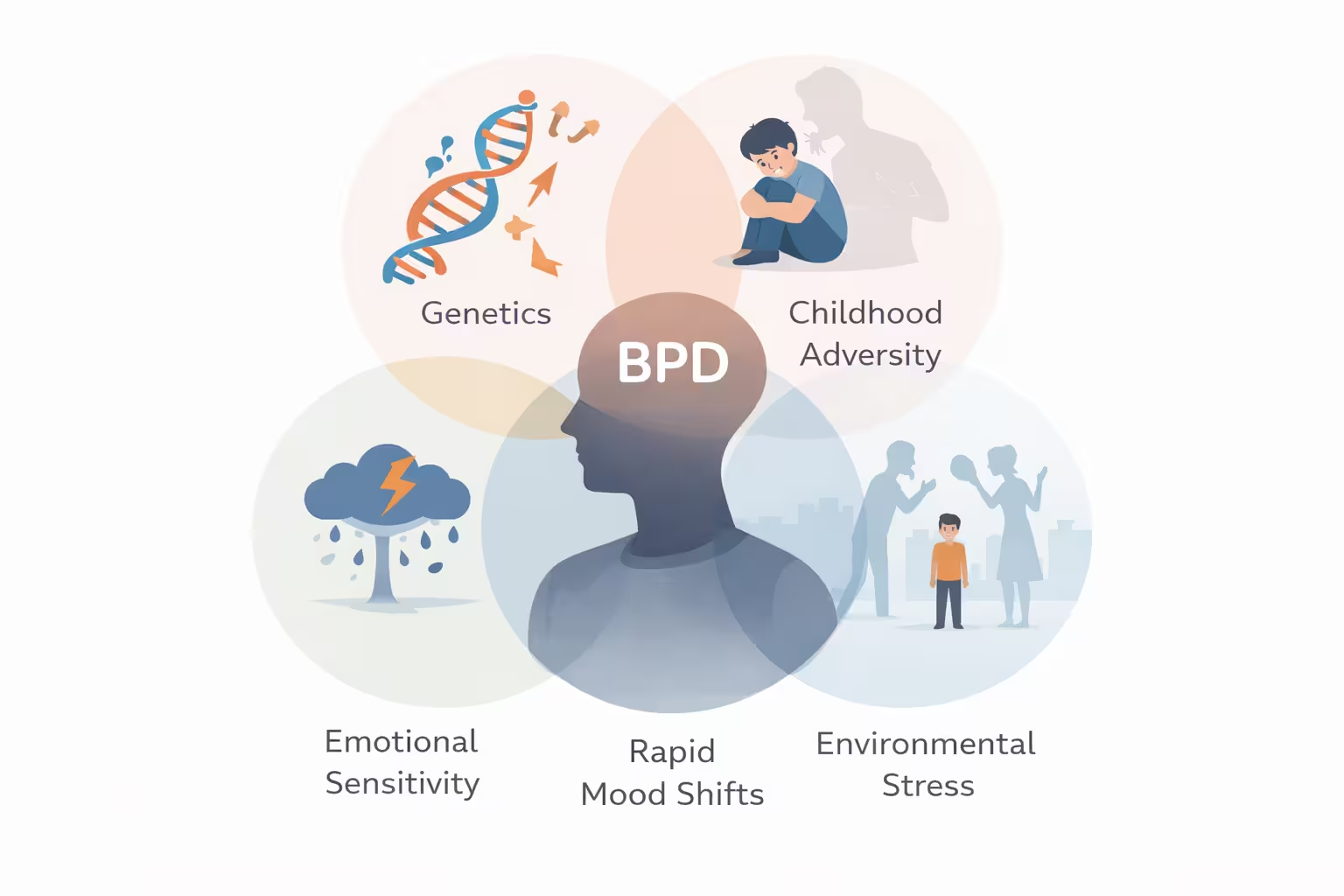
There is no single cause of borderline personality disorder. Current medical sources describe it as a condition shaped by a mix of biology, environment, and lived experience. Genetics appear to matter. Family history matters. So do adverse childhood experiences, disrupted attachment, family instability, abuse, neglect, or repeated loss. That does not mean everyone with trauma develops the disorder or that every person with the disorder has the same background. It means risk builds through a combination of factors rather than one simple cause.
Brain-based differences in emotion and behavior regulation may also play a role. NIMH notes that research continues to explore genetic and brain-based differences, along with cultural and social factors. This matters because the condition is not explained by willpower alone. It sits at the meeting point of temperament, stress response, learning history, and environment. For some people, high emotional sensitivity seems to meet an invalidating or unsafe environment, and that combination can make emotional control harder to develop in a steady way.
Risk does not look the same in every person. Some people mainly show anger and impulsivity. Others show emptiness, anxiety, withdrawal, or repeated relationship crises. Some appear high-functioning at work but fall apart in private. Others struggle in nearly every area. That difference matters because a person can suffer deeply without fitting the stereotype people expect. A careful evaluation should look at patterns across settings, not just one dramatic event or one hard relationship.
Why Borderline Personality Disorder Is Often Misunderstood
Borderline personality disorder carries heavy stigma. People may be labeled manipulative, impossible, or unstable without anyone asking what pain drives the behavior. That stigma can delay diagnosis and treatment. It can also make family members respond with blame instead of boundaries and support. The condition is real, distressing, and often linked with self-harm, sometime depression, anxiety, PTSD, eating disorders, bipolar disorder, ADHD, or substance use problems. When those conditions overlap, the picture becomes more confusing, and the person may receive partial treatment without enough focus on the full pattern.
Another point that gets missed is who gets diagnosed. MedlinePlus states that the disorder occurs equally in men and women, though women tend to seek treatment more often. Cleveland Clinic also notes that males may be equally affected but are sometimes misdiagnosed with conditions such as PTSD or depression. This matters in the United States because a public understanding built only around one presentation can leave many people unseen, especially those whose symptoms show up more as anger, substance use, or emotional shutdown. NIMH survey data found that 84.5% of adults with borderline personality disorder had at least one other mental disorder in the past year.
Borderline Personality Disorder vs. Bipolar Disorder
Many people confuse borderline personality disorder with bipolar disorder because both can involve impulsivity and mood changes. They are not the same. Cleveland Clinic explains that in BPD, mood and behavior can change rapidly in response to stress, especially interpersonal stress. In bipolar disorder, mood episodes are more sustained, often lasting days to weeks rather than hours, and they involve depressive or manic states. The difference matters because the treatment approach is not identical. A person can also have both conditions, which makes careful assessment essential.
A thorough clinician will look at triggers, timing, relationship patterns, identity problems, impulsivity, trauma history, and whether the person has clear manic or depressive episodes. Getting that distinction right often changes the entire treatment plan.
How Diagnosis Works

Diagnosing borderline personality disorder takes more than a checklist. There is no blood test or brain scan that confirms it. A mental health professional usually performs a detailed interview, reviews current symptoms, asks about earlier life experiences, studies relationship patterns, and checks for co-occurring conditions. The goal is not just to attach a label. It is to understand the full pattern, how severe it is, what risks are present, and what kind of treatment plan fits best. Recent APA guidance stresses a comprehensive, person-centered treatment plan and a collaborative discussion about diagnosis and care. Borderline personality disorder is usually diagnosed in late adolescence or early adulthood, although some people under 18 may be diagnosed when symptoms are severe and last at least a year.
Diagnosis can be emotionally difficult. Some people feel relief because the pattern finally makes sense. Others feel shame because of the stigma attached to the label. A good assessment should reduce fear, not increase it. It should explain what the diagnosis means, what it does not mean, what problems need urgent attention, and how treatment can help. Cleveland Clinic notes that providers often evaluate symptom severity early because that helps shape the treatment plan.
A careful evaluation often includes:
- Current symptoms and how long they have been present
- Relationship history and abandonment fears
- Self-image shifts and identity problems
- Impulse control and risky behavior
- History of self-harm, suicidal thoughts, or attempts
- Depression, anxiety, PTSD, bipolar disorder, ADHD, eating disorder, or substance use symptoms
- Physical health, social stress, and family history
- Cultural context and the person’s goals for treatment
Treatment Options That Actually Help
Borderline personality disorder can improve, and psychotherapy is the foundation of treatment. Multiple structured therapy approaches have evidence behind them. APA states that several structured psychotherapies are effective and that no single therapy has emerged as the only gold standard. Mayo Clinic, NIMH, and Cleveland Clinic also place talk therapy at the center of care. This is a major point because many people wrongly assume the condition cannot improve. In reality, the right therapy can reduce symptom severity, improve functioning, and make relationships more stable over time.

The best known approach is dialectical behavior therapy, often called DBT. It teaches practical skills for emotion regulation, distress tolerance, mindfulness, and relationship effectiveness. Other useful approaches include mentalization based therapy, schema therapy, cognitive behavioral therapy, and transference focused psychotherapy. Cleveland Clinic lists these as treatment options, and APA’s recent guidance supports structured psychotherapy that targets the core features of the condition. Different people respond to different formats, which is why treatment should be matched to the individual rather than forced into one model.
Medication has a more limited role. APA’s 2024 guidance says there is no evidence that medication effectively treats the core symptoms of the disorder, and Cleveland Clinic notes that medication is not usually the main treatment. Medicines may still be used for specific target symptoms or co-occurring conditions such as anxiety, depression, or bipolar disorder, but they should not replace therapy. This is one of the most important recent updates because it helps prevent long term overmedication without clear benefit.
What Happens in Therapy
Many people delay treatment because they do not know what therapy for borderline personality disorder actually looks like. In real life, it is often practical and structured. A therapist may help the person map triggers, identify patterns in conflict, slow down impulsive reactions, and practice ways to survive intense feelings without harming themselves or damaging relationships. Group work may be part of the plan, especially in DBT. Cleveland Clinic describes weekly therapy and group skill building as common parts of care. Over time, treatment aims to create a pause between feeling and action. That pause can change a life.
When Crisis Care or Hospital Care Is Needed
Some people need more support during a crisis. Short hospital stays may be recommended when safety is at risk, especially if there is serious self harm, suicidal behavior, or severe distress. That level of care is not a failure. It is a stabilizing step. NIMH and Cleveland Clinic both stress that people with the condition can be at higher risk of self harm and suicide, so safety planning is a real part of treatment, not an afterthought. In the United States, a person in immediate crisis can call or text 988 for the Suicide and Crisis Lifeline.
Living With Borderline Personality Disorder Day to Day
Living with borderline personality disorder often means managing intensity, not just symptoms. The hardest part is often not the label itself. It is the speed of reaction. A small event may create a large inner storm. That can affect sleep, appetite, work focus, spending, dating, and basic trust. This is why practical coping systems matter. A person may know what is rational and still feel unable to hold onto that knowledge in the moment. Treatment works best when it reaches daily life, not just the therapy room.
Helpful daily strategies often include a predictable sleep routine, reduced alcohol or drug use, regular meals, fewer high-conflict situations, emotional tracking, and clear plans for what to do during a trigger. Many people benefit from writing down warning signs that show a spiral is starting. These might include urges to check a partner’s phone, cut off a friend, spend impulsively, binge, self harm, or quit something suddenly. Naming the pattern early makes intervention more possible. The goal is not to feel nothing. The goal is to stay in control while feeling a lot.
A practical self-management plan may include
- A short list of personal triggers
- Early warning signs of escalation
- Two or three grounding tools that actually work
- One safe person to contact
- A therapy homework routine
- A limit on alcohol or substances during stressful periods
- A written crisis plan for nights, weekends, or breakups
Simple systems often work better than complex ones because they are easier to use when emotions are high.
Work, School, and Relationships
How a borderline personality disorder condition can make it hard to keep a job and can strain friendships, family ties, and marriage. At work or school, the pattern may show up as conflict with authority, fear of criticism, sudden quitting, burnout after rejection, or extreme reactions to feedback. In relationships, the deepest pain often comes from misreading closeness and distance. A person may want intimacy badly, then panic when intimacy feels risky. Understanding that pattern does not erase responsibility, but it does make the pattern easier to treat.
How Loved Ones Can Help Without Making Things Worse
Supporting someone with borderline personality disorder can feel exhausting if there are no boundaries. Mayo Clinic notes that if you notice symptoms in a family member or friend, you can encourage help, but you cannot force change. That idea is important. Loved ones help most when they stay calm, stay consistent, and avoid feeding cycles of rescue, blame, threat, and withdrawal. Validation matters. So do limits. “I can see you are hurting” is useful. So is “I will talk when we are both calmer.” Both can be true at the same time.
Helpful support often looks like this:
- Encourage treatment without arguing about the diagnosis every day
- Avoid insults, threats, and all-or-nothing language
- Set clear limits around abuse, violence, or manipulation
- Respond to crises seriously, especially self-harm threats
- Learn the person’s warning signs and safety plan
- Do not become the only source of support
- Consider therapy or support for yourself if the relationship is under strain
Loved ones are not therapists. Their job is steady support, not total emotional rescue.
Can Borderline Personality Disorder Improve Over Time
Borderline personality disorder can improve, often substantially. Mayo Clinic says many people get better with treatment. APA notes that most people experience reduced symptoms with treatment, though some symptoms may persist and some people need ongoing care. MedlinePlus also notes that symptoms may get better in or after middle age. Improvement does not mean a perfect life. It means fewer crises, safer behavior, more stable relationships, better functioning, and a stronger sense of self. That is a meaningful form of recovery.
Recovery is rarely linear. A person may do well for months, then struggle after loss, trauma, or relationship conflict. That does not erase progress. It simply means the condition is stress sensitive. The strongest long term outcomes usually come from a mix of skilled treatment, repeated practice, honest support, and time. The goal is not to become emotionless. The goal is to handle emotions without letting them destroy safety, identity, work, or connection.
Conclusion
Borderline personality disorder is not just about mood swings. It is a condition shaped by emotional pain, fear of loss, unstable self image, impulsive behavior, and intense relationship strain. It can look chaotic from the outside, but inside it often feels like trying to survive emotions that arrive too fast and hit too hard. Accurate diagnosis matters. Structured therapy matters. Family understanding matters. Most of all, the long term outlook is better than many people assume. With the right treatment and consistent support, many people build safer habits, steadier relationships, and a more stable life.
FAQs
What is borderline personality disorder?
Borderline personality disorder is a mental health condition that affects emotional regulation, relationships, self image, and impulse control. It often involves abandonment fears, unstable relationships, intense emotions, emptiness, anger, and risky behavior.
Is borderline personality disorder the same as bipolar disorder?
No. Both can involve mood changes and impulsivity, but bipolar disorder is a mood disorder with more sustained depressive or manic episodes. Borderline personality disorder is more closely tied to fast emotional shifts, relationship stress, and long standing patterns of coping and identity disturbance.
Can teenagers have borderline personality disorder?
Symptoms often start in adolescence or early adulthood. Cleveland Clinic notes that providers usually diagnose after age 18, though younger people may be diagnosed when symptoms are significant and last at least a year.
What is the best treatment for borderline personality disorder?
Psychotherapy is the main treatment. DBT is one strong option, but APA says several structured psychotherapies are effective and no single one is the only gold standard. Medication may help target specific symptoms or co occurring conditions, but it is not the main treatment for core symptoms.
Can borderline personality disorder get better?
Yes. Many people improve with treatment. Symptoms often become less severe over time, especially with structured therapy, safety planning, and steady support. Some people continue to need care, but meaningful recovery is common.
Why is borderline personality disorder often misdiagnosed?
The condition can overlap with depression, PTSD, anxiety, bipolar disorder, eating disorders, ADHD, and substance use problems. Men may also be misdiagnosed more often with PTSD or depression. That is why a detailed mental health assessment is important.
What should someone do during a crisis?
If there is immediate risk of suicide, self harm, or harm to others, emergency help is needed right away. In the United States, a person can call or text 988 for the Suicide and Crisis Lifeline. In a life threatening emergency, call 911.