Schizophrenia and Paranoid Schizophrenia: Symptoms, Differences & Treatment
Schizophrenia and paranoid schizophrenia are among the most severe and frequently misdiagnosed psychiatric conditions in the United States — yet for the approximately 3.5 million Americans living with these disorders, an accurate diagnosis is the single most transformative step toward recovery. Schizophrenia is a chronic psychotic disorder that disrupts how a person thinks, perceives reality, and functions in daily life. Its paranoid presentation — historically classified as a distinct subtype — is defined by persistent, unshakeable delusions (most often persecutory or grandiose) paired with auditory hallucinations, while leaving cognitive function comparatively intact. Understanding the difference between these two clinical profiles is not an academic exercise: it directly shapes treatment decisions, medication selection, prognosis, and the type of support a patient and their family will need for years to come.
Schizophrenia is not a character flaw or a failure of will. It is a brain disorder — as biological as diabetes — that responds to evidence-based treatment when caught early.”— Consistent position of the American Psychiatric Association (APA) and National Institute of Mental Health (NIMH)
Imagine hearing voices that no one else can hear, feeling certain that strangers are monitoring your every move, or believing that the government has planted a device inside your head. For millions of people living with schizophrenia and paranoid schizophrenia, these experiences are not imagined—they are terrifyingly real. Yet despite affecting approximately 24 million people worldwide according to the World Health Organization, these conditions remain among the most misunderstood in mental health.
This guide breaks down everything you need to know — from the biological roots and symptom profiles to the critical differences between schizophrenia subtypes, current treatment protocols, and how to support a loved one navigating this condition. Whether you are a patient, caregiver, student, or simply seeking clarity, this evidence-based resource is designed to give you real answers.
What Is Schizophrenia? A Clinical Overview
Schizophrenia is a severe, chronic psychiatric disorder characterized by disruptions in thought processes, perceptions, emotions, and behavior. It is classified under the broader category of psychotic disorders in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). The condition typically emerges in early adulthood — most commonly in the late teens to mid-30s — and tends to appear earlier in males than females.
Contrary to popular myth, schizophrenia does not mean a person has a ‘split personality.’ That misconception belongs to dissociative identity disorder, an entirely different condition. Schizophrenia instead involves a fractured relationship with reality itself—a break that can be episodic or chronic depending on the individual.
Core Diagnostic Criteria for Schizophrenia (DSM-5)
According to the DSM-5, a diagnosis of schizophrenia requires at least two of the following five symptoms for a significant portion of time during a one-month period, with signs persisting for at least six months:
- Delusions (fixed false beliefs)
- Hallucinations (most commonly auditory)
- Disorganized speech (incoherence, derailment)
- Grossly disorganized or catatonic behavior
- Negative symptoms (flat affect, alogia, avolition)
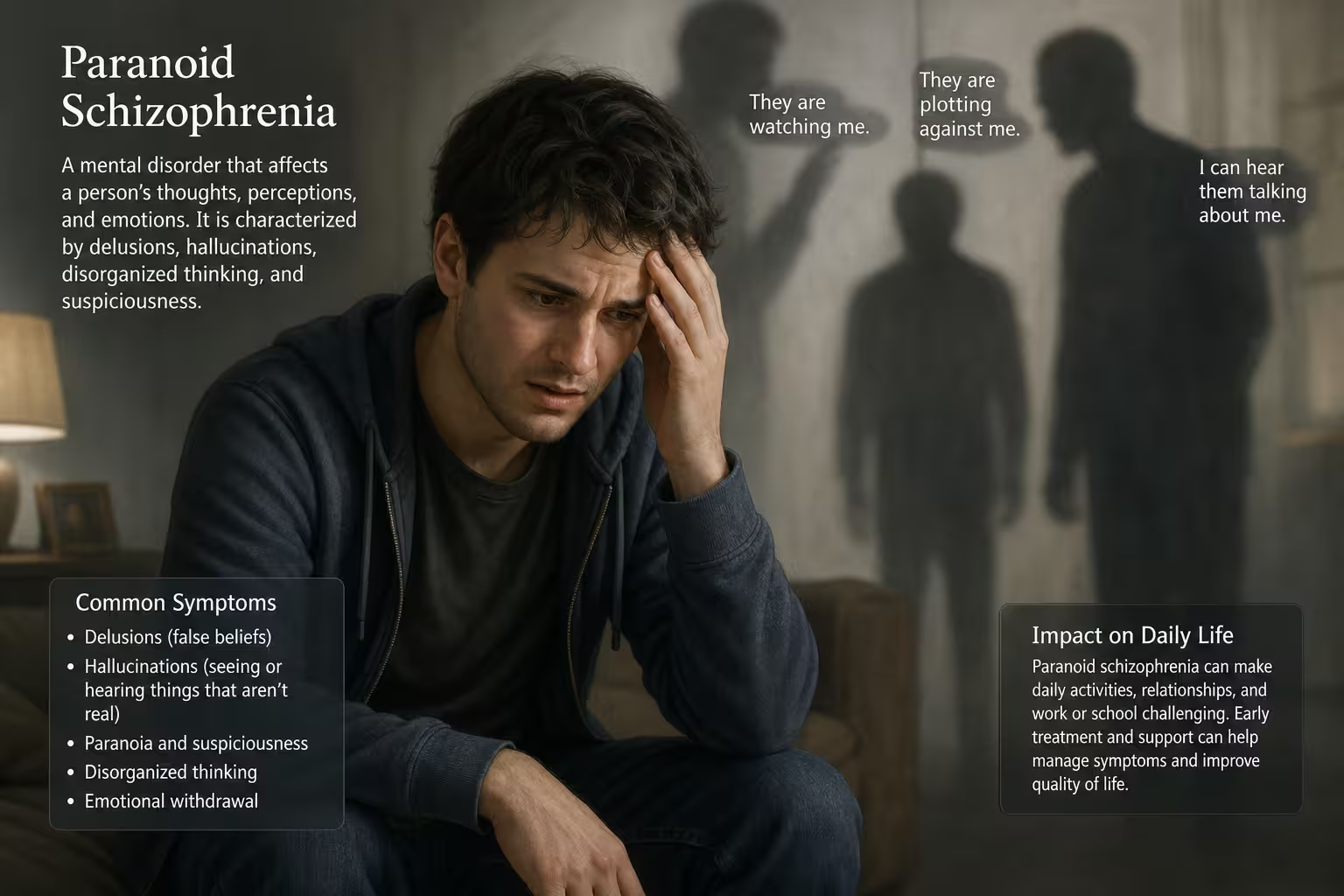
Understanding Paranoid Schizophrenia: What Sets It Apart?

Until the publication of the DSM-5 in 2013, paranoid schizophrenia was officially recognized as a distinct subtype of schizophrenia. Today, clinicians no longer use subtypes formally in the DSM-5, but the concept remains clinically relevant — and most mental health professionals still use the term to describe a specific symptom pattern.
In paranoid schizophrenia, the predominant features are persistent, elaborate delusions — often involving themes of persecution, grandiosity, or conspiracy — and frequent auditory hallucinations. The disorganized speech, flat affect, and catatonic behavior seen in other presentations of schizophrenia are typically less prominent. This is why many people with paranoid schizophrenia can appear relatively high-functioning on the surface, making the condition harder to detect.
Classic Paranoid Features at a Glance
|
Feature |
Description |
Example |
|
Persecutory Delusions |
Belief that others intend harm |
“My neighbors are poisoning my food” |
|
Grandiose Delusions |
Exaggerated sense of importance |
“I have been chosen to save the world” |
|
Referential Delusions |
Ordinary events carry personal meaning |
“The news anchor is speaking only to me” |
|
Auditory Hallucinations |
Hearing voices commenting or commanding |
Voices narrating one’s actions |
|
Hypervigilance |
Intense alertness to perceived threats |
Refusing to leave home due to fear |
Schizophrenia vs. Paranoid Schizophrenia: Key Differences
While schizophrenia and paranoid schizophrenia share a common diagnostic framework, understanding their differences helps patients and caregivers anticipate what to expect and seek appropriate care. Here is a side-by-side clinical comparison:
|
Category |
General Schizophrenia |
Paranoid Schizophrenia |
|
Dominant Symptoms |
Hallucinations, disorganized speech, negative symptoms |
Prominent delusions and auditory hallucinations |
|
Cognitive Function |
Often significantly impaired |
Relatively better preserved |
|
Emotional Expression |
Flat or blunted affect common |
Anger, anxiety, suspicion more typical |
|
Age of Onset |
Late teens to early 30s |
Typically later onset (mid-20s to 30s) |
|
Social Functioning |
Often severely impaired |
May function well in limited contexts |
|
Prognosis |
Variable; often poorer outlook |
Generally better long-term outcomes |
|
Insight into Illness |
Frequently poor |
May retain partial awareness |
Causes and Risk Factors: What Triggers These Conditions?
No single cause explains why some people develop schizophrenia while others do not. Current research points to a complex interplay of genetic, neurobiological, and environmental factors. Understanding these risk factors can inform early intervention and reduce stigma by framing mental illness as a medical condition rather than a personal failing.
1. Genetic Vulnerability
Genetics play a significant role. If one parent has schizophrenia, their child faces approximately a 10% lifetime risk — compared to roughly 1% in the general population. If both parents are affected, that risk climbs to about 40%. A 2022 study in Nature Genetics identified over 270 genetic loci associated with schizophrenia risk, highlighting the complexity of its hereditary component.
2. Neurobiological Factors
Brain imaging studies have consistently shown structural differences in individuals with schizophrenia, including enlarged lateral ventricles, reduced gray matter volume in the prefrontal cortex, and abnormalities in hippocampal structure. The dopamine hypothesis — long central to understanding psychosis — proposes that overactivity of dopamine transmission in the mesolimbic pathway drives positive symptoms like delusions and hallucinations.
3. Prenatal and Early-Life Factors
Exposure to infections, malnutrition, or extreme stress during pregnancy has been linked to higher schizophrenia risk in offspring. Being born in winter or spring also slightly elevates risk, potentially due to seasonal viral exposure during prenatal development. Complications during birth, including oxygen deprivation, are additional documented risk factors.
4. Environmental and Psychosocial Triggers
Childhood trauma, urban upbringing, and migration have all been associated with elevated risk. Substance use — particularly cannabis use during adolescence — is one of the most studied environmental triggers. A large meta-analysis found that heavy cannabis users had approximately double the risk of developing a psychotic disorder compared to non-users.
Recognizing the Symptoms: Early Warning Signs and Clinical Stages
Schizophrenia rarely appears suddenly. It typically unfolds in identifiable stages, and recognizing these phases early dramatically improves treatment outcomes. Clinicians describe three broad phases: prodromal, active, and residual.
|
Phase |
Duration |
Key Signs |
Who Recognizes It? |
|
Prodromal |
Months to years |
Social withdrawal, declining grades/work performance, odd beliefs, sleep disruption |
Family, teachers, close friends |
|
Active (Acute) |
Weeks to months |
Full psychotic symptoms — hallucinations, delusions, disorganized speech |
Mental health professionals, emergency services |
|
Residual |
Ongoing between episodes |
Lingering negative symptoms, cognitive difficulties, social withdrawal |
Psychiatrists, outpatient care teams |
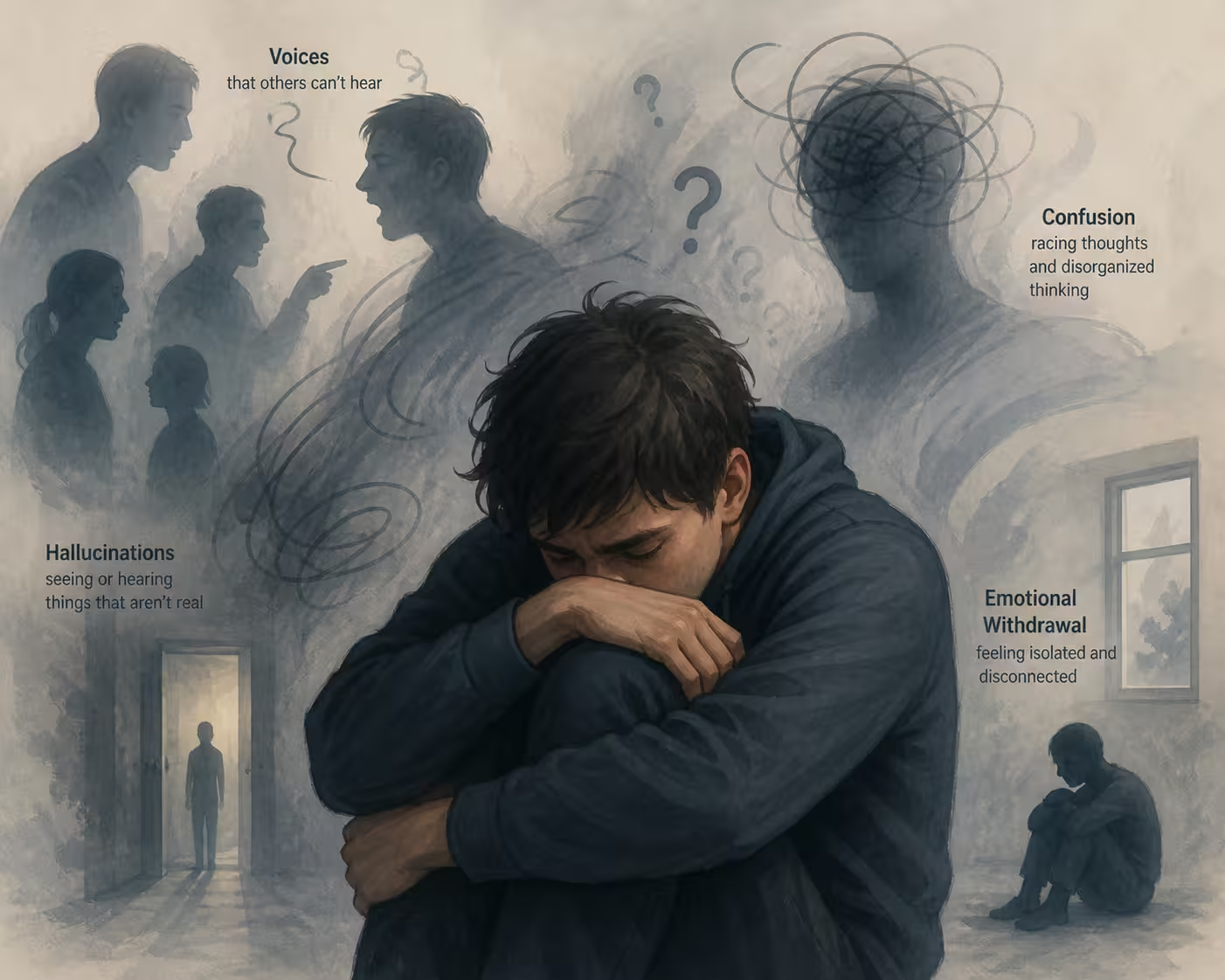
Positive vs. Negative Symptoms
Mental health professionals divide schizophrenia symptoms into two major categories. Understanding this distinction is crucial because they respond differently to treatment.
|
Symptom Type |
What It Means |
Examples |
|
Positive Symptoms |
Experiences ADDED to baseline reality |
Hallucinations, delusions, disorganized thinking, agitation |
|
Negative Symptoms |
Experiences REMOVED from baseline functioning |
Flat affect, poverty of speech, lack of motivation, anhedonia |
|
Cognitive Symptoms |
Impairments in mental processing |
Poor working memory, trouble concentrating, difficulty planning |
In paranoid schizophrenia specifically, positive symptoms tend to dominate, while negative symptoms are comparatively mild. This is one reason why individuals with this pattern may go undiagnosed longer — they appear engaged and can carry on conversations, even while holding bizarre beliefs.
How Is Schizophrenia Diagnosed?
There is no single blood test or brain scan that diagnoses schizophrenia. Diagnosis is clinical — based on a thorough psychiatric evaluation, medical history review, and the exclusion of other potential causes. Clinicians must rule out medical conditions (thyroid disorders, epilepsy, brain tumors), substance-induced psychosis, bipolar disorder with psychotic features, and other psychiatric conditions before confirming a schizophrenia diagnosis.
A complete diagnostic workup typically includes a structured psychiatric interview, standardized rating scales such as the Positive and Negative Syndrome Scale (PANSS), neuroimaging (usually MRI) to rule out organic causes, laboratory tests, and collateral history from family members. Diagnosis should never be rushed — the DSM-5 requires symptoms to persist for at least six months before a schizophrenia diagnosis is confirmed.
Treatment Options for Schizophrenia and Paranoid Schizophrenia
Treatment for schizophrenia and paranoid schizophrenia is most effective when it combines medication, psychotherapy, and community support. While there is currently no cure, sustained treatment enables many individuals to lead meaningful, productive lives.
Antipsychotic Medications: First-Line Treatment
Antipsychotic medications are the cornerstone of schizophrenia treatment. They work primarily by blocking dopamine receptors, reducing positive symptoms like hallucinations and delusions. Clinicians generally categorize antipsychotics into two generations:
|
Generation |
Examples |
Targets |
Notable Side Effects |
|
First-Generation (Typical) |
Haloperidol, Chlorpromazine, Fluphenazine |
Dopamine D2 receptors |
Extrapyramidal symptoms (tremors, stiffness), tardive dyskinesia |
|
Second-Generation (Atypical) |
Risperidone, Olanzapine, Clozapine, Aripiprazole, Quetiapine |
Dopamine + Serotonin receptors |
Weight gain, metabolic syndrome, sedation |
|
Long-Acting Injectables (LAI) |
Paliperidone palmitate, Aripiprazole lauroxil |
Same as oral equivalents |
Injection site discomfort; improved adherence |
Clozapine deserves special mention: it is the only antipsychotic proven effective for treatment-resistant schizophrenia. However, it requires regular blood monitoring due to the risk of agranulocytosis (a dangerous drop in white blood cells).
Psychosocial Interventions
Medication alone is rarely sufficient. Evidence strongly supports combining pharmacotherapy with structured psychosocial treatments:
- Cognitive Behavioral Therapy for Psychosis (CBTp): Helps patients examine and challenge delusional beliefs and develop coping strategies for hallucinations.
- Family Therapy and Psychoeducation: Reduces relapse rates by improving family communication, reducing expressed emotion, and equipping caregivers with practical tools.
- Supported Employment (Individual Placement and Support model): Helps individuals return to or enter competitive employment with ongoing vocational support.
- Social Skills Training: Addresses deficits in interpersonal functioning, which are especially impactful in the long-term course of illness.
- Assertive Community Treatment (ACT): An intensive team-based outreach model for individuals with severe illness who struggle to engage with traditional services.
Early Intervention Programs
One of the most significant developments in schizophrenia care is the push for early intervention in psychosis (EIP). Programs such as Coordinated Specialty Care (CSC) — supported by SAMHSA in the United States — combine low-dose medication, CBT, family support, and supported education for young people experiencing their first episode. Research shows that early intervention can delay or prevent full-blown schizophrenia in some cases and leads to significantly better long-term outcomes.
Living with Paranoid Schizophrenia
Daily life with paranoid schizophrenia presents challenges that go far beyond managing symptoms. Many individuals face difficulties with housing security, employment discrimination, social isolation, and navigating a healthcare system that can feel complex and overwhelming. The rate of comorbid depression in schizophrenia is estimated at around 25–50%, and the condition carries a significantly elevated risk of suicide — approximately 5–6% of individuals with schizophrenia die by suicide.
Medication adherence is one of the most critical factors in long-term stability. Studies estimate that up to 50% of patients with schizophrenia do not take their medications as prescribed, often due to lack of insight (anosognosia), side effects, or financial barriers. Long-acting injectable antipsychotics have emerged as a valuable solution for those who struggle with daily oral medication routines.
Supporting a Loved One with Paranoid Schizophrenia
Caring for someone with paranoid schizophrenia can be emotionally exhausting, particularly when the person directs their paranoid beliefs toward the caregiver. Here are evidence-based strategies for navigating this:
- Do not argue about or confirm delusional beliefs — acknowledge the person’s feelings without reinforcing the delusion.
- Maintain calm, predictable routines — structure reduces anxiety and the sense of threat that fuels paranoia.
- Learn to recognize early warning signs of relapse — changes in sleep, increasing agitation, or social withdrawal often precede acute episodes.
- Access caregiver support — organizations like NAMI (National Alliance on Mental Illness) offer family education programs and peer support.
- Prioritize your own mental health — caregiver burnout is real and requires active prevention.
Schizophrenia Statistics in the United States
Understanding the scope of these conditions in the American context helps contextualize their public health significance:
|
Statistic |
Figure |
Source |
|
Estimated U.S. adults with schizophrenia |
~3.5 million (approx. 1.1% of population) |
NIMH |
|
Average age of onset (males) |
Late teens to mid-20s |
DSM-5 / APA |
|
Average age of onset (females) |
Late 20s to early 30s |
DSM-5 / APA |
|
Lifetime suicide risk |
5–6% |
Journal of Psychiatric Research |
|
Treatment gap (untreated schizophrenia) |
~50% in the U.S. |
WHO Global Mental Health Atlas |
|
Annual cost burden (direct + indirect) |
Over $155 billion |
Cloutier et al., 2016 |
|
Adherence to antipsychotic medication |
~50% long-term adherence |
Velligan et al. meta-analysis |
Emerging Research and Future Directions
The field of schizophrenia research is moving rapidly. Several areas offer genuine promise for improving outcomes in the coming decade:
Glutamate-based treatments: While dopamine blockade has driven antipsychotic therapy for decades, researchers are increasingly targeting the glutamate system — particularly NMDA receptor dysfunction — which may underlie cognitive and negative symptoms that current medications poorly address.
Biomarkers and precision psychiatry: Researchers are working to identify reliable biological markers (genetic, neuroimaging, inflammatory) that could predict individual medication response, reducing the current trial-and-error process in treatment selection.
Digital therapeutics: Smartphone-based monitoring tools and digital CBT programs are being studied as adjuncts to standard care, particularly for improving adherence and early relapse detection.
Anti-inflammatory approaches: Mounting evidence implicates neuroinflammation in schizophrenia pathology. Clinical trials exploring anti-inflammatory agents, including aspirin and omega-3 fatty acids, as adjunct treatments are ongoing.
Frequently Asked Questions
Conclusion
Schizophrenia and paranoid schizophrenia are serious, often misunderstood conditions that affect millions of Americans and their families. Yet with accurate diagnosis, consistent treatment, and strong community support, the trajectory of these illnesses can be profoundly altered. What was once considered a hopeless diagnosis now carries a far more nuanced — and often hopeful — prognosis for those who receive timely, comprehensive care.
If you or someone you love is experiencing symptoms of psychosis, seek evaluation from a qualified mental health professional without delay. Early intervention remains the single most powerful tool available. And above all, remember: schizophrenia does not define a person — it is one part of a much larger, richer human story.
Medical Disclaimer: This article is for informational purposes only and does not constitute medical advice. Always consult a licensed mental health professional for diagnosis and treatment recommendations.