Paranoid Schizophrenia Symptoms: Signs, Stages, and What They Really Mean
Imagine hearing a voice call your name in an empty room, or feeling — with absolute certainty — that strangers on the street are watching your every move. For millions of people living with paranoid schizophrenia, these experiences are not imagination. They are as real and vivid as anything in the physical world. Yet despite how common this condition is, most people still do not fully understand what it looks, sounds, and feels like from the inside.
This article goes beyond surface-level definitions. It offers a detailed, clinically grounded exploration of paranoid schizophrenia symptoms—from the earliest warning signs to the more complex cognitive and emotional changes that develop over time. Whether you are a concerned family member, a caregiver, or someone seeking answers about your own mental health, the information here is designed to guide you with clarity and compassion.
Understanding Paranoid Schizophrenia
Schizophrenia is a chronic, serious mental disorder that affects approximately 1 in 100 people worldwide, according to the World Health Organization. Paranoid schizophrenia — historically one of the most recognized subtypes — is characterized by persistent delusions and auditory hallucinations, typically without the severe disorganization of thought or flat affect seen in other presentations.
It is worth noting that the DSM-5 (Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition), published by the American Psychiatric Association in 2013, removed the formal subtype classification. Clinicians now diagnose simply ‘schizophrenia’ along a spectrum of severity. However, the term ‘paranoid schizophrenia’ remains widely used because it accurately describes a presentation where paranoid thinking and persecutory delusions are the dominant features.
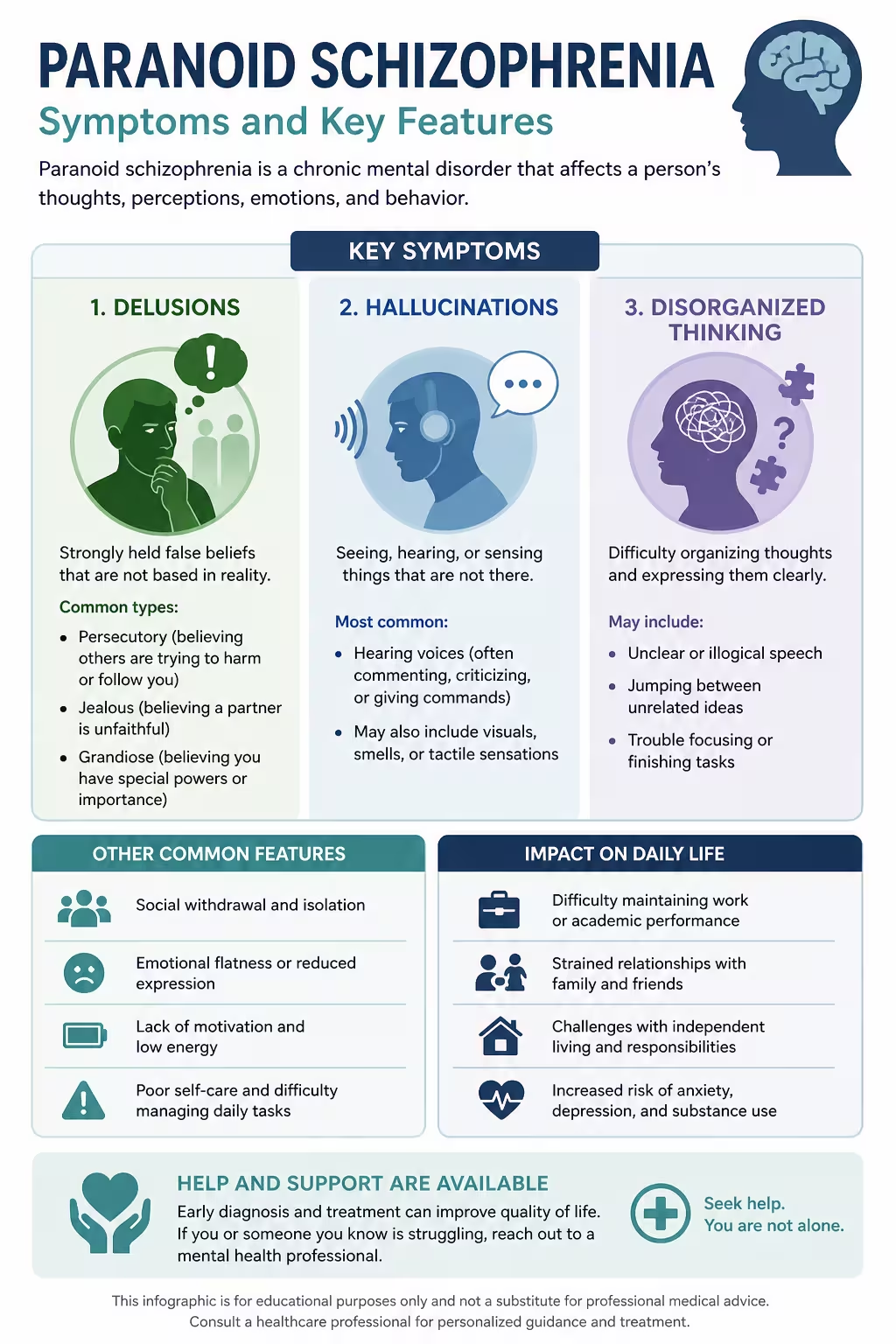
Understanding these distinctions matters because it affects how symptoms are recognized, how treatment is tailored, and how families can best offer support. The core paranoid schizophrenia symptoms include three major categories: positive symptoms, negative symptoms, and cognitive symptoms.
Positive Symptoms of Paranoid Schizophrenia
In clinical language, ‘positive’ does not mean good. It refers to symptoms that add an experience that would not normally be there — thoughts, perceptions, and behaviors that are disconnected from reality. These are often the most dramatic and recognizable features of the disorder.
Persecutory Delusions
Delusions are fixed, false beliefs that do not change even when presented with contradicting evidence. In paranoid schizophrenia, persecutory delusions are the most common type. The person may believe they are being followed by government agents, poisoned by neighbors, watched through their television, or targeted by an organized group.
These are not fleeting worries. They are deeply held convictions. A person experiencing persecutory delusions may stop eating because they fear their food is being tampered with. They may cover windows, disconnect electronics, or avoid certain streets due to the certainty that danger is near. The distress involved is profound and completely genuine to the person experiencing it.
Other types of delusions that appear in paranoid presentations include:
- Referential delusions — believing random events (a news broadcast, a passerby’s comment) are directly referencing or meant for them
- Grandiose delusions — an inflated belief in one’s own power, identity, or mission (e.g., believing they are a prophet or possess special knowledge)
- Delusions of control — the conviction that an outside force is controlling their thoughts, feelings, or body movements
- Thought insertion or withdrawal — believing that thoughts are being placed into or removed from their mind by an external entity
Auditory Hallucinations
Among all forms of hallucinations, auditory hallucinations — hearing voices or sounds that others cannot — are by far the most common in paranoid schizophrenia symptoms. Research published in Schizophrenia Bulletin estimates that up to 70–80% of people with schizophrenia experience auditory hallucinations at some point.
These voices may speak directly to the person, offer a running commentary on their actions, issue commands, or argue with one another. Some voices are recognized as familiar; others are completely unknown. Critically, these voices feel externally generated — they seem to come from outside the person’s own mind. This is why they are so disorienting and why dismissing them as ‘just in your head’ is both inaccurate and unhelpful.
A smaller proportion of people also experience visual hallucinations (seeing things that aren’t there), tactile hallucinations (physical sensations without a cause), or olfactory hallucinations (smelling things others cannot detect). These tend to occur alongside auditory experiences rather than in isolation.
Disorganized Thinking and Speech
While more pronounced in other presentations of schizophrenia, disorganized thinking can still emerge as a paranoid schizophrenia symptom. This includes rapidly shifting from one topic to another (known as ‘loosening of associations’ or ‘derailment’), making connections between unrelated ideas, or communicating in ways that become difficult for others to follow.
In some cases, a person may exhibit ‘word salad’ — speech that is so fragmented it becomes meaningless. Even when communication remains relatively intact, there is often an underlying looseness in logical reasoning, particularly around the subject of their delusions.
Negative Symptoms: The Silent Side of Paranoid Schizophrenia
Negative symptoms are among the least discussed and least recognized aspects of schizophrenia. Where positive symptoms add experiences, negative symptoms remove them — stripping away normal functions that were once present. These are often more disabling in the long term than the dramatic positive symptoms.
Affective Flattening and Emotional Withdrawal
Affective flattening refers to a marked reduction in emotional expression. The person’s face may appear expressionless; their voice may lose its natural variation in tone. Eye contact becomes rare. Emotional responses to news — good or bad — appear muted or absent. This is not indifference; it is a symptom. The internal emotional world may still exist, but the outward expression is dampened.
Emotional withdrawal can follow, with the person pulling back from relationships, social events, and activities that previously brought them pleasure. This withdrawal is often misinterpreted as stubbornness, depression, or simply not caring — when in reality it reflects the neurological and psychological impact of the illness.
Avolition: Loss of Motivation and Drive
Avolition is the inability to initiate and sustain goal-directed activity. A person with this symptom may sit for hours without engaging in any productive activity — not because they are lazy, but because the drive to begin tasks has been significantly impaired. Personal hygiene may be neglected. Meals may be skipped. Appointments may be missed repeatedly.
This can be one of the most frustrating paranoid schizophrenia symptoms for families to witness, especially because it does not look like illness from the outside. It often looks like a choice. Understanding that avolition is a symptom — not a character flaw — is critical to maintaining a compassionate and supportive relationship with a loved one.
Alogia and Anhedonia
Alogia refers to poverty of speech — brief, empty replies and difficulty generating thoughts to speak. When asked a question, a person experiencing alogia may respond with a single word or not at all. This is different from being quiet by nature; it reflects a reduction in the internal generation of language and thought.
Anhedonia — the loss of pleasure from activities once enjoyed — is another significant negative symptom. Hobbies, music, social connection, even food may no longer produce any emotional reward. This symptom significantly overlaps with depression and is one reason why depression and schizophrenia are frequently co-occurring conditions.
Cognitive Symptoms
Cognitive impairments associated with paranoid schizophrenia are perhaps the most underreported of all symptom categories. Research consistently shows that cognitive symptoms are among the strongest predictors of functional outcomes — meaning they significantly affect a person’s ability to work, maintain relationships, and live independently.
Working Memory and Attention Deficits
Working memory — the ability to hold and use information over short periods — is frequently impaired in schizophrenia. A person may forget mid-sentence what they were trying to say, lose track of a task, or have difficulty following multi-step instructions. Attention deficits mean that conversations require more effort, and sustained focus on work or study becomes exhausting.
A landmark study published in the Archives of General Psychiatry found that cognitive impairment in schizophrenia is present even before the first psychotic episode, suggesting these changes are part of the core neurobiology of the disorder rather than a side effect of medication or chronic illness.
Executive Function Difficulties
Executive function encompasses planning, decision-making, problem-solving, and the ability to adjust behavior based on feedback. In paranoid schizophrenia, executive function is often significantly reduced. The person may struggle to plan meals, manage finances, navigate bureaucratic tasks, or respond flexibly to new situations. These impairments are invisible to the outside world but deeply limiting in daily life.
Processing Speed and Social Cognition
Reduced processing speed means the person takes longer to interpret information and formulate responses. Social cognition — the ability to read facial expressions, understand tone of voice, and interpret the intentions of others — is also impaired. This makes social interaction confusing and exhausting. Misreading social cues can reinforce paranoid interpretations, creating a cycle where cognitive symptoms and positive symptoms amplify each other.
Early Warning Signs
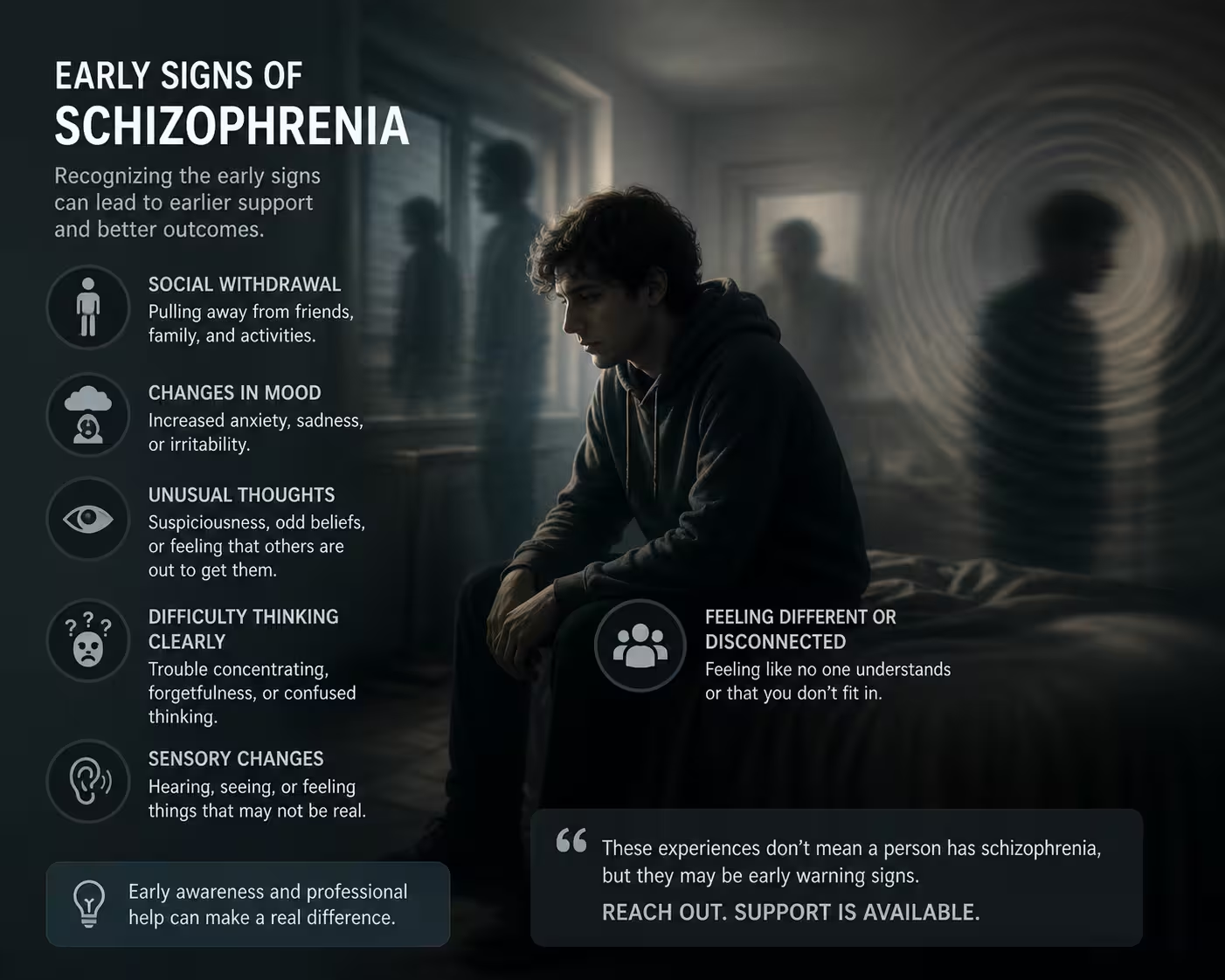
Before the first full psychotic episode, most people with schizophrenia go through a period called the prodrome — a phase that may last months to years. During this time, symptoms are subtle, and the person may still function reasonably well. Identifying this phase is crucial because early intervention significantly improves long-term outcomes.
Studies show that reducing the ‘duration of untreated psychosis’ (DUP) — the time between first psychotic symptoms and treatment — is one of the strongest predictors of recovery. Earlier treatment leads to better results.
Common early warning signs include:
- Social withdrawal — pulling away from friends and family without obvious reason
- Declining academic or work performance — a noticeable drop in functioning that cannot be explained by external stressors
- Increased suspiciousness — growing mistrust of people in their life, including close family members
- Unusual perceptual experiences — brief or fleeting sensory experiences that feel strange or unreal
- Disrupted sleep patterns — significant changes in sleeping habits, often combined with increased anxiety
- Odd beliefs or magical thinking — beginning to express ideas that seem unusual or hard to follow
- Neglect of hygiene — a gradual reduction in self-care without explanation
These signs do not confirm a diagnosis on their own. However, when several appear together — especially in someone between the ages of 16 and 30, when schizophrenia most commonly first appears — they warrant prompt clinical evaluation.
How Paranoid Schizophrenia Is Diagnosed
There is no single blood test, brain scan, or imaging study that definitively diagnoses schizophrenia. Diagnosis is clinical, made by a qualified mental health professional through a comprehensive evaluation of symptoms, history, and functional impairment.
According to the DSM-5, a diagnosis requires:
- Two or more of the following core symptoms for at least one month: delusions, hallucinations, disorganized speech, grossly disorganized or catatonic behavior, or negative symptoms
- At least one of the two symptoms must be delusions, hallucinations, or disorganized speech
- Significant functional decline in work, relationships, or self-care
- Continuous signs of the disturbance for at least six months
- Ruling out other causes such as substance use, medical conditions, or mood disorders with psychotic features
The diagnostic process often includes structured clinical interviews, neuropsychological testing, medical history review, and sometimes brain imaging to rule out organic causes such as brain tumors, autoimmune encephalitis (particularly anti-NMDA receptor encephalitis, which can closely mimic schizophrenia), or neurological conditions.
What Causes Paranoid Schizophrenia? Risk Factors and Neurobiology
The exact cause of schizophrenia remains one of psychiatry’s most studied and debated questions. The consensus is that it arises from a complex interaction of genetic, neurobiological, and environmental factors — not any single cause alone.
Genetic Factors
Schizophrenia has a strong genetic component. The risk is approximately 10% for first-degree relatives (parents, siblings, or children) of someone with the diagnosis, compared to about 1% in the general population. For identical twins, if one twin has schizophrenia, the other has a roughly 48% risk — underscoring that genes are influential but not deterministic.
Brain Structure and Dopamine Dysregulation
Neuroimaging studies have consistently found differences in brain structure and function in people with schizophrenia, including reduced grey matter in the prefrontal cortex and enlarged ventricles. The dopamine hypothesis — one of the most established neurobiological theories — proposes that excess dopamine activity in certain brain pathways contributes to positive symptoms like delusions and hallucinations.
Glutamate dysregulation has also emerged as a significant factor. The NMDA receptor hypofunction model suggests that reduced glutamatergic signaling contributes to both negative and cognitive symptoms, which may explain why antipsychotic medications (primarily dopamine blockers) address positive symptoms more effectively than negative or cognitive ones.
Environmental Risk Factors
Several environmental factors increase the risk of developing schizophrenia, particularly in genetically predisposed individuals:
- Prenatal exposure to infections, malnutrition, or stress
- Complications during birth (e.g., oxygen deprivation)
- Growing up in urban environments
- Cannabis use during adolescence, particularly high-potency varieties
- Childhood trauma and adverse experiences
- Migration and minority stress
Treatment Options

Paranoid schizophrenia is a chronic condition, but it is far from untreatable. With appropriate and sustained care, many people achieve significant reductions in symptom severity and lead meaningful, productive lives.
Antipsychotic Medications
Antipsychotic medications remain the cornerstone of treatment for paranoid schizophrenia symptoms. They are divided into two generations:
- First-generation (typical) antipsychotics — such as haloperidol and chlorpromazine, developed in the 1950s-60s. Effective against positive symptoms but carry higher risks of movement-related side effects (tardive dyskinesia, extrapyramidal symptoms).
- Second-generation (atypical) antipsychotics — such as risperidone, olanzapine, quetiapine, aripiprazole, and clozapine. Generally better tolerated and somewhat more effective against negative symptoms, though metabolic side effects (weight gain, diabetes risk) require monitoring.
Long-acting injectable (LAI) formulations of antipsychotics have become increasingly important for people who struggle with daily oral medication. LAIs improve medication adherence and are associated with lower rates of relapse and hospitalization.
Psychosocial Interventions
Medication alone is rarely sufficient. The most effective treatment models combine pharmacological and psychosocial approaches:
- Cognitive Behavioral Therapy for Psychosis (CBTp) — evidence-based therapy that helps individuals examine and reframe delusional beliefs, develop coping strategies for voices, and reduce distress. Recommended by the National Institute for Health and Care Excellence (NICE) for all people with schizophrenia.
- Family Psychoeducation — structured programs that educate families about the illness, reduce expressed emotion (a significant relapse trigger), and improve communication. Studies show it reduces relapse rates by up to 50% when sustained.
- Social Skills Training — targeted therapy to address deficits in social cognition and interaction, helping individuals navigate relationships and employment.
- Supported Employment (IPS model) — the Individual Placement and Support model has strong evidence for helping people with schizophrenia gain and maintain competitive employment.
- Assertive Community Treatment (ACT) — an intensive, team-based model that brings treatment to the person rather than requiring clinic attendance. Particularly effective for those with frequent hospitalization.
First Episode Psychosis Programs
Coordinated Specialty Care (CSC) programs — such as the widely studied NAVIGATE and EASA programs in the United States — provide multidisciplinary, recovery-oriented treatment immediately following a first psychotic episode. Research published in the American Journal of Psychiatry found that CSC significantly outperformed standard care in improving quality of life, symptoms, and community functioning.
Living With Paranoid Schizophrenia
Recovery from paranoid schizophrenia does not always mean the complete absence of symptoms. For many people, recovery means building a meaningful life despite ongoing challenges — maintaining relationships, pursuing goals, and finding stability through consistent treatment.
Peer support has emerged as a powerful component of recovery. Programs staffed by people with lived experience of psychosis provide both practical guidance and an irreplaceable sense of being understood. Organizations such as NAMI (National Alliance on Mental Illness) and Mental Health America offer peer-led support groups, helplines, and educational resources across the United States.
Stress management is also critical. Stress is a well-established trigger for psychotic relapse. Sleep hygiene, exercise, structured routines, and the avoidance of alcohol and cannabis all reduce relapse risk. For caregivers, setting clear boundaries, attending to their own mental health, and joining caregiver support groups are equally essential.
Frequently Asked Questions
Conclusion
Paranoid schizophrenia symptoms span a wide spectrum — from the vivid, terrifying experiences of delusions and auditory hallucinations to the quiet, often invisible erosion of motivation, emotion, and cognitive function. No two people experience this condition in exactly the same way, and that complexity is precisely why awareness, nuanced understanding, and individualized care matter so deeply.
If you recognize these signs in yourself or someone you love, the most important step is not to wait. Early intervention, the right combination of medication and psychosocial support, and a compassionate network of care can change the trajectory of this illness. Schizophrenia is not a life sentence — it is a condition that, with sustained and evidence-based care, can be managed, adapted to, and lived well with.





