Anxiety Symptoms, Causes, Types, Treatment, and When to Get Help
You can feel your chest tighten before a big interview. You can lose sleep before a test. You can replay a hard conversation in your head for hours. That is part of being human. But when fear, dread, and constant worry stop acting like a warning system and start running your life, the issue may be bigger than everyday stress. In the United States, about 19 percent of adults have an anxiety disorder in a given year, and around 31 percent experience one at some point in life. That is not rare. It is common, disruptive, and treatable.
People feel high when they are actually not.
Anxiety at a Glance
|
Topic |
Quick Answer |
|
What it is |
A mental and physical response to perceived threat, stress, or uncertainty |
|
When it becomes a problem |
When fear or worry is frequent, excessive, hard to control, and starts affecting daily life |
|
Common signs |
Restlessness, racing thoughts, sleep problems, muscle tension, rapid heartbeat, avoidance |
|
Main types |
Generalized anxiety disorder, panic disorder, social anxiety disorder, phobias |
|
Main causes |
Genetics, stress, trauma, brain chemistry, personality factors, medical triggers |
|
Common treatments |
Therapy, medication, lifestyle changes, stress management techniques |
|
When to get help |
When symptoms interfere with work, relationships, sleep, health, or daily function |
Key Takeaways
- Anxiety can be normal, but it becomes a disorder when it is persistent and disruptive
- Symptoms can affect the mind, body, behavior, and sleep
- Different anxiety disorders have different trigger patterns
- Treatment often includes therapy, medication, or both
- Avoidance usually makes anxiety worse over time
- Early help often leads to better outcomes
What anxiety actually is
At its core, anxiety is the mind and body preparing for threat. Your heart may beat faster. Your breathing may change. Your muscles may tighten. Your stomach may react. Your thoughts may narrow around danger, uncertainty, or worst-case outcomes. In a real risk situation, that response can help. It is part of the same protective system often called fight or flight. The problem starts when that response shows up too often, lasts too long, or fires in situations that are not truly dangerous.
That is why the question is not “Do you ever feel anxious?” Almost everyone does. The better question is whether your fear or worry has become persistent, out of proportion, and disruptive. The American Psychiatric Association makes this distinction clearly. Normal nervousness comes and goes. A disorder keeps returning or stays long enough to interfere with daily life. When you begin avoiding normal activities, losing function, or shaping your life around fear, the issue has crossed a meaningful line.
When normal worry becomes a disorder
A useful way to judge the difference is to look at three things. First, how often it happens. Second, how intense it feels. Third, how much it interferes with life. If you feel keyed up before one presentation, that is ordinary. If you spend weeks dreading meetings, avoid speaking, lose sleep, and start turning down opportunities, that points in another direction. Clinical concern rises when symptoms are not brief and situational but persistent, recurring, and life-limiting.
Another clue is avoidance. People often think the problem is the fear itself. In reality, avoidance is what makes it stronger over time. When you stop driving, flying, attending events, answering calls, going to class, or leaving home because of dread, your world shrinks and the fear gets reinforced. Many top-ranking pages mention this, but not strongly enough. It is one of the most important real-life markers because it tells you the problem is not just internal discomfort. It is changing behavior and reducing freedom.
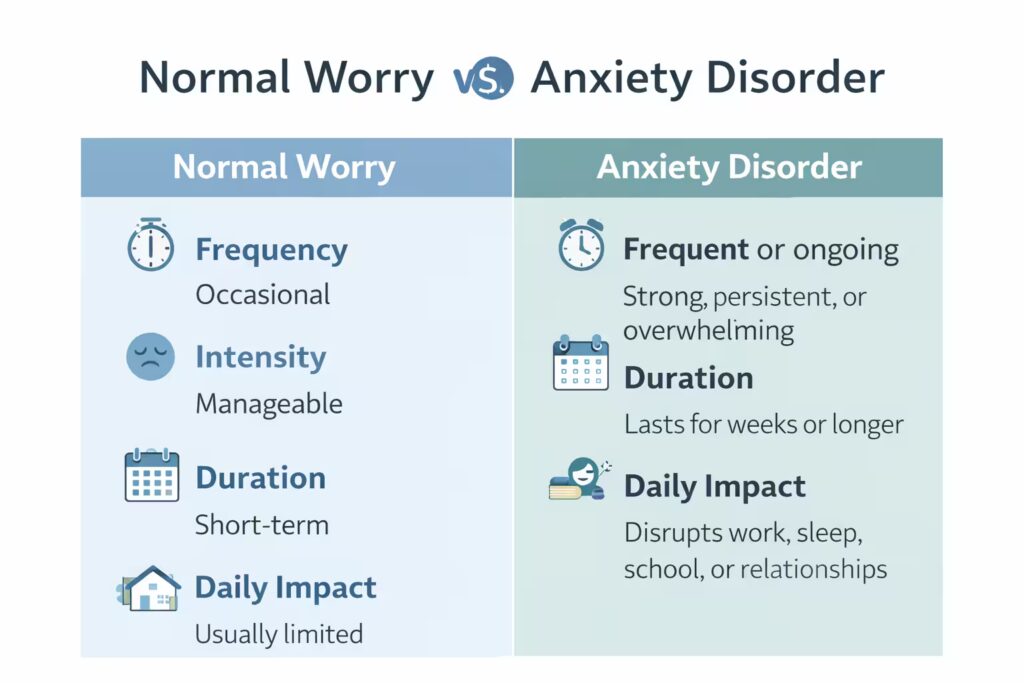
Normal Worry vs Anxiety Disorder
|
Factor |
Normal Worry |
Anxiety Disorder |
|
Frequency |
Occasional |
Frequent or ongoing |
|
Trigger |
Usually linked to a clear event |
May happen with or without a clear reason |
|
Intensity |
Manageable |
Strong, persistent, or overwhelming |
|
Duration |
Short-term |
Lasts for weeks or longer |
|
Daily impact |
Usually limited |
Disrupts work, sleep, school, or relationships |
|
Control |
Easier to calm down |
Feels hard to stop or manage |
|
Behavior change |
Little to none |
Leads to avoidance or major lifestyle changes |
Common types people need to understand
This topic is not one single condition. It is a group of related disorders. The main types commonly highlighted by U.S. medical sources include generalized anxiety disorder, panic disorder, social anxiety disorder, and phobia-related disorders. Some sources also include separation anxiety disorder, agoraphobia, PTSD, and OCD in broader statistics or related groupings, though classification language can vary depending on the source and context.
Generalized anxiety disorder is the pattern of broad, hard-to-control worry across everyday areas like health, work, money, family, or routine responsibilities. Panic disorder centers on repeated panic attacks and fear of having more of them. Social anxiety disorder involves intense fear of scrutiny, judgment, or embarrassment in social or performance situations. Phobia-related disorders focus on strong fear tied to specific objects, situations, or environments, like flying, heights, needles, enclosed spaces, or being unable to escape easily. Each type feels different, which is why broad articles that blur them together lose precision.
Main Types of Anxiety Disorders
|
Type |
What It Usually Looks Like |
Common Trigger |
|
Generalized anxiety disorder |
Constant worry about everyday life, even when there is no major threat |
Work, money, health, family, future |
|
Panic disorder |
Sudden waves of intense fear with strong physical symptoms |
Can happen unexpectedly or after stress |
|
Social anxiety disorder |
Strong fear of judgment, embarrassment, or rejection |
Speaking, meeting people, eating in public |
|
Specific phobias |
Intense fear of a particular object or situation |
Heights, flying, needles, animals, enclosed spaces |
|
Agoraphobia |
Fear of situations where escape feels difficult |
Crowds, travel, open spaces, public places |
|
Separation anxiety |
Distress when away from a loved one or safe person |
Distance, travel, school, change |
Signs and symptoms you should not ignore
Symptoms can be psychological, physical, and behavioral. That mix is exactly why people often miss what is happening. They assume the problem is digestive, cardiac, hormonal, or just “me being dramatic.” In reality, fear-driven body changes can be intense. Mayo Clinic and Cleveland Clinic both list a mix of mental and physical signs, including feeling nervous or on edge, trouble concentrating, restlessness, muscle tension, racing heart, sweating, trembling, shortness of breath, sleep disruption, nausea, tingling, and digestive upset.
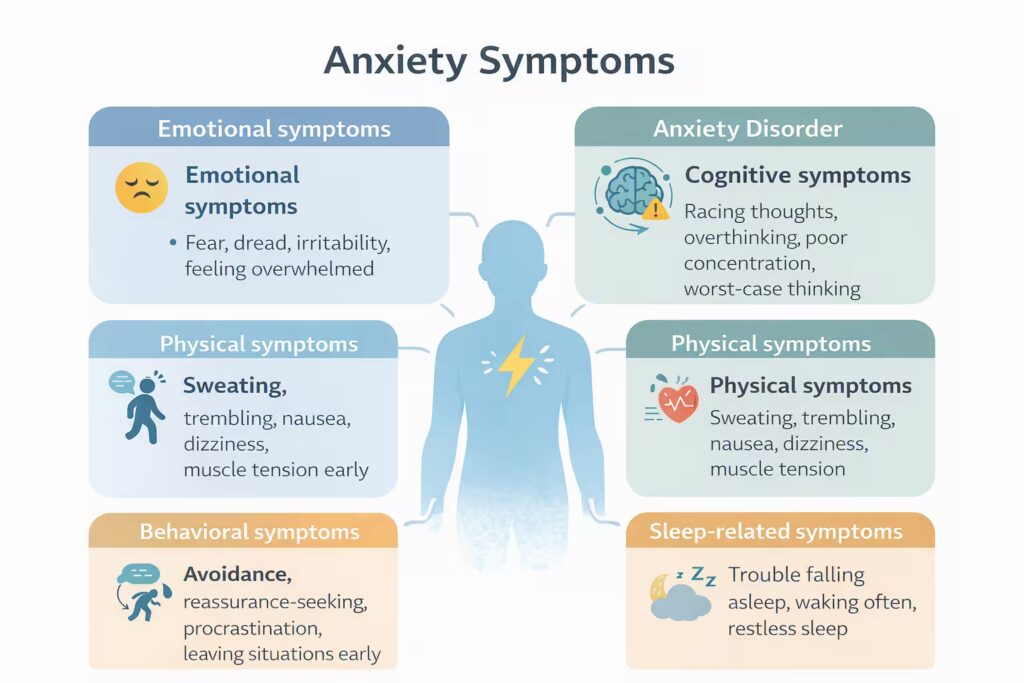
Common warning signs include:
- Persistent worry that feels hard to control
- A sense of dread, danger, or doom
- Restlessness or feeling constantly keyed up
- Racing heartbeat, chest tightness, sweating, or shaking
- Difficulty sleeping or staying asleep
- Trouble concentrating because your mind keeps circling back to fear
- Avoiding places, people, tasks, or situations that trigger symptoms
- Digestive discomfort, nausea, or stomach upset with no clear cause
What catches many people off guard is how physical this can feel. Someone may say, “I’m not worried. I just can’t breathe properly, my hands shake, and my chest hurts.” That still fits the picture. Mental distress does not always announce itself as a thought first. Sometimes the body gets there before the mind can name it. That is one reason people end up in urgent care or the emergency room, convinced they are having a medical crisis. Sometimes it is a panic attack. Sometimes it is not. That is why symptoms should never be self-diagnosed with arrogance.
Panic attacks are not the whole story
Many people use panic attacks and anxiety as if they are identical. They are not. A panic attack is a sudden surge of intense fear with strong physical symptoms, often including chest pain, pounding heart, sweating, trembling, dizziness, nausea, or a sense that something catastrophic is happening. Some people have occasional panic attacks under extreme stress without meeting criteria for panic disorder. Panic disorder involves repeated attacks and ongoing worry or behavioral changes because of them.
This matters because panic symptoms can look like serious medical problems. Mayo Clinic explicitly notes that panic attack symptoms can resemble a heart attack and advises medical evaluation if you are not sure what is causing them. That is not fearmongering. It is basic safety. Chest pain, breathlessness, fainting, or new severe symptoms should not be brushed off because a blog told you it was probably “just panic.” That kind of lazy advice gets people hurt.
What causes anxiety
There is no single cause. The evidence points to a mix of biology, life experience, and environment. Cleveland Clinic notes that neurotransmitters and hormones are involved, that brain circuits such as the amygdala play a role in fear processing, and that genetics and long-term stress can increase risk. NIMH also points to environmental and genetic contributors and ongoing research into how symptoms can shift after trauma, illness, pregnancy, and major life changes.
Risk does not mean destiny. A family history can raise the odds, but it does not guarantee you will develop a disorder. Trauma can raise vulnerability, but not every person with trauma develops the same pattern. Chronic illness, severe life stress, and long periods of uncertainty can also push the nervous system toward a more reactive state. That is why simplistic content that blames only “negative thinking” is weak. The real picture is broader. Biology, learning, stress history, and coping patterns interact.
Lifestyle factors can make symptoms worse even when they are not the root cause. Excess caffeine can intensify physical signs. Poor sleep lowers emotional resilience. Heavy alcohol use can temporarily numb distress and then worsen it. Nicotine and stimulant-heavy products can also keep the body revved up. None of this means you caused your condition with coffee or a bad night of sleep. It means the nervous system is sensitive, and daily habits can either calm it or keep feeding it.
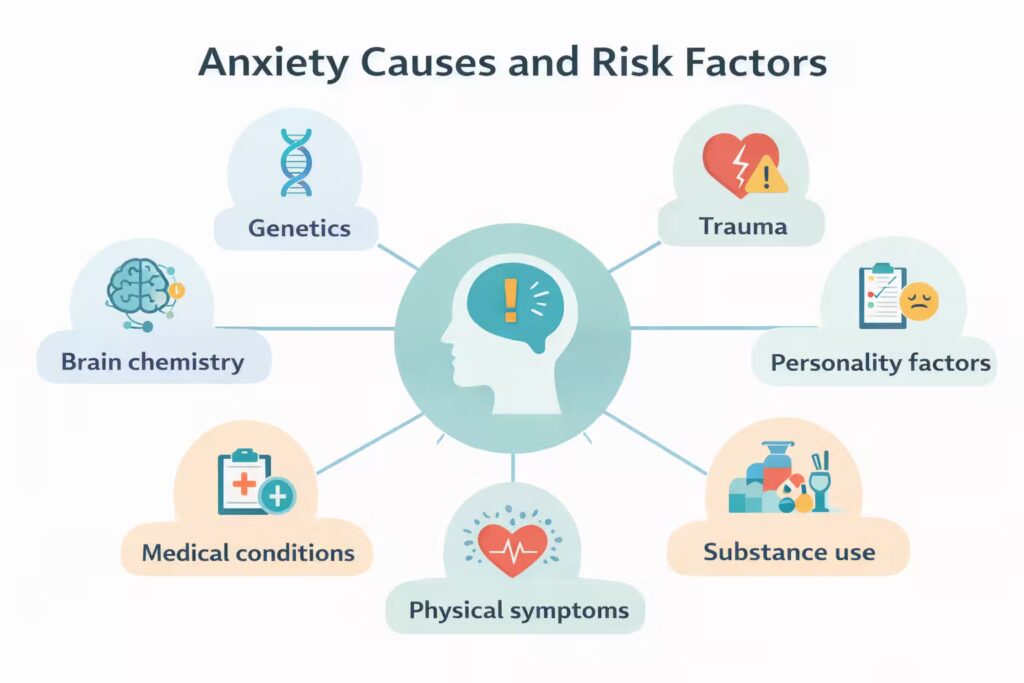
Possible Causes and Risk Factors
|
Factor |
How It Can Contribute |
|
Genetics |
Family history can increase risk |
|
Brain chemistry |
Imbalances in stress and mood regulation may play a role |
|
Trauma |
Past traumatic events can keep the body in a heightened alert state |
|
Chronic stress |
Long-term pressure can overload coping systems |
|
Perfectionism, sensitivity, and fear of uncertainty can increase vulnerability |
|
|
Medical conditions |
Some illnesses or hormone issues can trigger similar symptoms |
|
Substance use |
Caffeine, alcohol, nicotine, or drug use can worsen symptoms |
What can look like anxiety but is not
This is one of the biggest gaps in weaker articles. Not every racing heart, dizziness spell, stomach issue, or trembling episode comes from mental distress. Physical conditions can mimic or worsen symptoms. Cleveland Clinic and Mayo both note that medical evaluation may be needed to rule out underlying causes. Thyroid problems, medication effects, sleep deprivation, stimulant use, hormone shifts, substance use, and some heart or breathing issues can all complicate the picture.
That does not mean every symptom requires a battery of tests. It means serious or new symptoms deserve proper evaluation, especially when the pattern is sudden, severe, or unusual for you. Good clinical care does not assume “it’s all in your head.” It checks. Then, if physical causes are ruled out, treatment can focus more confidently on the mental health side. Readers need this section because it prevents two common mistakes: ignoring real medical issues and endlessly chasing medical tests for a condition that actually needs psychological care.
How diagnosis works in real life
Diagnosis is not made through a blood test or a brain scan. Providers look at the pattern of symptoms, how long they have been happening, how severe they are, and how much they disrupt daily life. Cleveland Clinic notes that mental health professionals use DSM-5 criteria and also consider sleep, behavior, medical history, family history, medications, and whether symptoms interfere with normal functioning. Mayo Clinic similarly describes an assessment process that may start with primary care and then move to a mental health specialist if needed.
A competent evaluation also looks for overlap. Depression, substance misuse, trauma-related symptoms, and other mental health conditions can exist alongside anxiety. That overlap is common and can complicate diagnosis. This is another place where thin content fails. It tells readers to “talk to your doctor” without explaining what the doctor is actually trying to figure out. The real goal is to determine whether the symptoms fit a defined disorder, whether something medical is contributing, and which treatment path makes the most sense.
The most effective treatments
The main evidence-based treatments are psychotherapy, medication, or a combination of both. This is consistent across major U.S. sources including NIMH, Mayo Clinic, and the American Psychiatric Association. The strongest first-line psychotherapy is usually cognitive behavioral therapy, or CBT. It helps people identify distorted patterns of thought, change unhelpful reactions, and reduce avoidance. For phobias and other fear-driven patterns, exposure-based work is often part of that process.
CBT matters because it does more than provide emotional support. It teaches a skill set. You learn how to challenge catastrophic predictions, tolerate bodily sensations without spiraling, and re-enter situations you have started avoiding. Mayo Clinic describes CBT as the most effective form of psychotherapy for anxiety disorders, and NIMH calls CBT the gold standard for conditions like social anxiety disorder. That is why content that spends half the article on vague self-care and two lines on therapy is not serious enough.
Medication can also be useful, especially when symptoms are moderate to severe, persistent, or making therapy hard to engage in. NIMH notes that SSRIs and SNRIs are commonly used for depressive and anxiety disorders and are often preferred because they generally have fewer side effects than older antidepressants. APA also notes that SSRIs are commonly used as first-line medication options for several anxiety disorders. These drugs do not “fix your personality.” They target symptom systems that are keeping the nervous system stuck in overdrive.
Short-term medications have a place, but people need the truth about them. NIMH and Mayo both note that benzodiazepines may be used for short-term relief in limited circumstances, but they are not intended as a long-term answer because tolerance, dependence, and withdrawal issues can become real problems. Beta-blockers may help with physical symptoms like shaking or rapid heartbeat in some situations, but they do not treat the core thought and fear cycle.

What treatment feels like in the first weeks
This is another section most competitor pages underplay. People quit too early because they expect fast relief. Psychotherapy takes practice. Medication takes time. NIMH states that antidepressants often take around four to eight weeks to show fuller effects, and some problems such as sleep, appetite, energy, or concentration may shift before mood or worry fully improves. Mayo Clinic also notes that finding the right treatment can take some trial and error. That is frustrating, but it is normal.
Early treatment can even feel awkward before it feels useful. In therapy, you may be asked to face thoughts or situations you have been avoiding. With medication, you may worry about side effects or misread every sensation in the first week as proof it is “not for you.” This is exactly why guided care matters. Improvement is often gradual, not dramatic. The target is not emotional numbness. The target is better function, less avoidance, improved sleep, fewer spirals, and more control over daily life.
What Helps and What Makes Anxiety Worse
|
Often Helps |
Often Makes It Worse |
|
Regular sleep |
Sleep deprivation |
|
Physical activity |
Sitting still all day with built-up tension |
|
Structured routines |
Chaotic schedules |
|
Therapy homework and gradual exposure |
Avoidance |
|
Limiting caffeine |
Excess caffeine and energy drinks |
|
Healthy coping tools |
Alcohol misuse or constant reassurance-seeking |
|
Calm breathing and grounding |
Doomscrolling and constant threat monitoring |
What you can do day to day
Self-management is not a substitute for professional care when symptoms are severe. But it does matter. The best daily tools are boring, repetitive, and effective. That is the truth. There is no mystical hack here. You want to reduce nervous system load and stop reinforcing fear. Major clinical sources point to stress management, regular exercise, better sleep habits, limiting caffeine and alcohol, and using structured relaxation techniques such as breathing exercises and mindfulness.
A useful daily plan includes:
- Keeping wake and sleep times consistent
- Reducing excess caffeine, nicotine, and alcohol
- Moving your body most days, even with a short walk
- Practicing slow breathing or relaxation before symptoms peak
- Writing down worry patterns instead of letting them run unchecked
- Limiting avoidance by taking small, planned steps toward feared tasks
- Staying in treatment long enough to judge it fairly
One point needs to be blunt. Many people say they “tried everything” when what they actually tried was irregular sleep, doomscrolling, caffeine overload, reassurance-seeking, and one breathing video. That is not a treatment plan. Real self-management is structured, repeated, and tied to measurable behavior. The goal is not to never feel fear for anything big again. The goal is to stop building your life around it.
How this affects work, school, and relationships
This condition is often minimized because it is invisible. But its effects are not small. NIMH states that symptoms can interfere with job performance, schoolwork, and relationships. APA notes the same pattern. In real life, that can mean missed deadlines, overpreparation, irritability, constant checking, trouble making decisions, exhaustion from poor sleep, avoidance of meetings or social events, and repeated reassurance-seeking that strains close relationships.
Social damage is especially under-discussed. Some people appear high-functioning because they still show up, but the cost is huge. They rehearse conversations for hours, avoid speaking, turn down invitations, hide symptoms, or carry constant dread behind ordinary tasks. Others look “lazy” or “uncommitted” when they are actually stuck in a fear cycle. Good content should say this clearly because readers often do not recognize impairment until they see their daily behavior described plainly.
Children, teens, and adults do not always show it the same way
Age matters. NIMH notes that research increasingly looks at how symptoms and treatment needs change across life stages and after major life events. Adolescents are affected in large numbers too. NIMH reports that about 31.9 percent of U.S. adolescents have had an anxiety disorder, with higher prevalence among females than males. In children and teens, symptoms may show up as irritability, school refusal, reassurance-seeking, physical complaints, or social withdrawal rather than polished adult-style descriptions of worry.
Adults may hide symptoms better, but that does not mean the disorder is milder. In some adults it shows up as perfectionism, controlling behavior, overworking, health worries, repeated checking, or chronic tension that gets mistaken for personality. Older adults may focus more on health concerns or life stability. The pattern changes, but the core issue stays the same. Fear becomes too frequent, too broad, too intense, or too costly. Content that ignores age differences misses a real search need and loses relevance.
When to get help
Get professional help if symptoms are persistent, getting worse, or interfering with sleep, work, school, relationships, or daily functioning. Mayo Clinic states plainly that getting help earlier can make treatment easier than waiting until the problem becomes severe. Cleveland Clinic also notes that seeking treatment early can reduce disruption and complications. That advice is practical, not dramatic. People usually wait too long. They keep telling themselves they should be able to handle it alone. That delay often deepens the pattern.

Seek urgent medical evaluation when symptoms could reflect a medical emergency, especially chest pain, severe shortness of breath, fainting, or a first-time episode that feels extreme and unfamiliar. If someone is in immediate danger, call 911. If you are in the United States and need crisis support for mental health, emotional distress, substance use, or suicidal thoughts, call or text 988 or use the 988 chat service. SAMHSA states that 988 is available 24/7 across the United States and connects people with trained crisis counselors.
What recovery really looks like
Recovery is rarely a straight line. Symptoms can improve and still flare during stress, illness, conflict, grief, or major life transitions. That does not mean treatment failed. It means the nervous system is being tested again. The realistic goal is not permanent emotional calm. The goal is faster recovery, less avoidance, better judgment, better sleep, and the ability to keep living even when discomfort shows up. Most reputable clinical sources agree that treatment helps many people live normal, productive lives.
The biggest mindset shift is this. You do not win by waiting to feel perfectly safe before acting. You improve by learning that discomfort can be tolerated, questioned, and reduced over time. That is what therapy teaches. That is what gradual exposure proves. That is why recovery is less about eliminating every fearful thought and more about changing your relationship to those thoughts and the behaviors that follow them. Once you grasp that, the condition starts to look less mysterious and more manageable.
Frequently Asked Questions
Conclusion
Anxiety is common, but common does not mean trivial. It can range from useful short-term alertness to a serious disorder that narrows your life, drains your body, and reshapes your decisions. The difference comes down to persistence, intensity, and impairment. The strongest evidence-backed path forward is not denial, endless reassurance, or vague “positive thinking.” It is proper assessment, therapy that addresses fear and avoidance, medication when appropriate, and daily habits that stop feeding the cycle. If symptoms are disrupting your life, stop minimizing them. Get them evaluated and treat the problem for what it is.